
The CFS – Chronic Fatigue Syndrome webpage
for CFS/Physical – where the main aspect is the abnormal physiological response to physical exertion ©
The research project of 1982-4 which proved a physical basis for the fatigue can be seen here My publications, and newspaper reports about that research can be seen here, and my talks here.
My new essay on the symptoms, cause, diagnosis and treatment of CFS is here.
My webpage which contains a brief summary of the treatment methods which I developed between 1975 and 1983, and which are now evident all around the world today, can be seen here.
See also the Worlds best CFS research here.
Tens of thousands of South Australians would have heard about my chronic fatigue research between 1982 and1983, and since, when I was interviewed on radio, or spoke on talk back radio programs, or from my letters and articles published in local and state newspapers or journals, and hundreds of thousands of people would have learnt about it all over Australia, and overseas,from newspaper reports and journal articles published in interstate and internationally based, and or, internationally distributed journals, and if anyone decided to copy my methods and claim them to be their own, it would have been relatively easy to find out more, and it has recently become apparent to me, in 2012, that it is what has happened. See a summary of my publications here, and my talks
To compound that aspect, two anonymous editors managed to convince other editors that I was a worthless, non-notable, fringy kook who only participated as a sports technician in one small, insignificant research project, and whose ideas were nonsense and rubbish, and arranged for me to be banned from Wikipedia.
The simple fact is that I solved a major problem related to exercise and chronic fatigue, and anyone who tried to use different methods in the future would not succeed.
|
in order to treat my own health problems in 1976 I was told to ignore my symptoms and run faster and faster, until I regained my former fitness (see my report here). However I had many adverse responses to that process, so I decided to invent my own methods of exercise. It has become apparent to me, since November 2012, that a London researcher named Simon Wessely has been copying me, but instead of asking me to be a consultant, and paying me the appropriate fee, he has chosen to use other patients as human guinea pigs at their risk, to determine and verify everything that I already knew, so that he could take all the credit for the discoveries AND the verification for himself. I have also learned that other people are copying my methods without knowing that the ideas were mine, or without mentioning my name. Needless to say, the copy is never as good as the original. (they are summarised here and later here, and many of my methods have not been published) |
My research is a century ahead of the PACE trialsWhen you read the report below which lists all of the problems that the PACE trial is having, I would like you to consider that I invented the method and already know how to prevent those problems. Unlike the PACE trial which had difficulty recruiting patients, I didn’t, because I decided to join an exercise class myself, not because I was told, and the PACE trial had problems with people dropping out of the course, but I didn’t, because it was my idea, and when I had problems I kept solving them, and the only reason I stopped after 10 months was because I injured my knee cartilage, not because of the problems with exercise. I also continued to study the problems in the 30 years since, so I don’t have to LOOK FORWARD to find solutions to the problems because I now have the benefit of hindsight from thousands of personal experiments. There is nothing about the ailment which is a mystery to me, and I can effectively prevent, relieve, or control all of the symptoms Massive problems with the PACE trials faulty copies of my researchIn 1975 the treatment offered by my doctor was not having any effect at relieving my various ailments so I decided to study them myself. One of my earliest attempts was to join an exercise class where I spent almost a year experimenting on methods of improving my fitness, and a few years later I was reading research journals and books when I found that the world’s top researchers were having trouble getting patients to exercise. In 1982 the head of a research institute asked me to design a program to solve that problem, and when his research cardiologists too busy on other projects to do the study he asked me to organise it. The first 3 months of the program was successful, and was followed by a second which was reported in major newspapers all around Australia. I was then asked to increase the study to 200 patients to have a major influence on world opinion but I was still having problems with my own health so I declined. However, I continued to experiment on my own health for the next 2 decades before I was able to get a reliable and efficient understanding of the problems. I have found out recently that Simon Wessely of London began coping my methods from 1987 onwards, and other researchers have been following my essays and books, and reports on my website, and when I improved the details in the description of symptom control in 2008, which I have since called The Banfield Principles, Wessely’s colleague Peter White started a five year study of 650 patients with CFS and exercise called the PACE trial. When it was finished and published patients started complaining about all of the problems it caused with 51% reporting that they were worse after the training than before. My following ocmments are about a further report entitled: LETTER – Chronic fatigue treatment trial – PACE trial authors’ reply to letter by Kindlon) in the BMJ website dated 15th October 2013 (BMJ 2013; 347 doi: http://dx.doi.org/10.1136/bmj.f5963. The discussion includes the words “BEYOND PACE – MOVING THE DEBATE FORWARD” and has suggestions of “the need for a new debate now” (end of quote) This was one of the statements “This was a pragmatic trial to help patients while there is no other treatment available … The study was carefully conducted in the manner of a drug intervention study” (end of quote) My comment: there was no treatment at all available in 1975, and the modern authors are not mentioning that I developed the exercise/lifestyle regimes that are being used and discussed today??? The article also states “Perhaps this brings us back to PACE for some basic insight . . . Although there are probably well over a hundred Support Groups and a dozen or so ME charities in the UK, this trial experienced considerable recruitment difficulty, taking about a year longer than planned.” (end of quote) My comment: My research from 1976 to 1982 is where insight into this ailment “originally” came from, not the PACE trial, and I know why they are having considerable difficulty with recruitment. They also state . . . “In order to avoid awkward looking calculations down the road, clearly you do not want anyone leaving the trial.” (end of quote) My comment: I know why people are leaving the trial.” They also state . . . “Trialists must presumably plan very carefully to ensure they eliminate the problem of loss as far as possible, just as I imagine that is how one would proceed when identifying suitable candidates for a drug trial, who won’t kill your desired results. I would also expect that some pharmaceutical companies might get a bit nervous over yet more independent trials of their products. But in order to prevent loss, how does one communicate to candidates that which might be involved in this instance?” (end of quote) The article further states . . . “There is some evidence to suggest that being on benefits and/or income protection (IP) are poor prognostic factors as they are contingent upon the patient remaining unwell … Address blocks to recovery, e.g. being in receipt of benefits … If participants are insistent that there is an ongoing “physical” problem, it is rarely helpful to directly challenge them on this point” (end of quote) My comment: being on benefits or not did not play any part in the research of 65 patients in 1982, and it is irrelevant to why people won’t train. They also state “it is interesting and perhaps rather unsurprising that the CBT withdrawals and losses were almost twice those of Adaptive Pacing Therapy and Graded Exercise Therapy” (end of quote) My final comment: The developers of the PACE trial do not have sufficient understanding of the problems to prevent or fix them. |
I have had the symptoms of chronic fatigue for 38 years, since 1975, and wrote my observations, theories, and methods of managing the fatigue in the first four years. There is no cure, but, because of the accuracy of my methods, I haven’t had severe fatigue since, and I don’t take pills.
See a current report by Mike Wennergren who describes his own chronic fatigue on 18-8-13, and also comments on an economist named Roger King who estimates that he spent $8000 on medical bills in one year and calculates that the illness has cost him more than $1,6 million, including income he’s been forced to forgo. See here
Needless to say I could have saved him a lot of time, trouble, and money.
Wennergren now does one of the things that I knew 37 years ago, and recommended in my 1982 research project – he used to participate in triathlons, but now has to limit his activities carefully and rest several times during the day. See my report here.
I can also say that it doesn’t matter whether you are educated or uneducated, rich or poor, you can still get the chronic fatigue syndrome, and money doesn’t make it go away, but it would improve the patients quality of life.
|
I developed the world’s first scientific method for diagnosing chronic fatigue with exercise testing. In order to treat my own chronic fatigue I enrolled in an exercise program at the South Australian Institute for Fitness Research and Training in 1976. Within a year I was able to determine, on the basis of scientifically reliable results that, at the start my own aerobic capacity was abnormally low, and that, with regular exercise my fitness level improved in three months and then stopped improving despite increasing the amount and frequency of exercise, which scientifically proved that I had an impaired capacity for exercise, and that it was chronic. Seven years later I was asked to design and co-ordinate a research project to assess the problem on a larger scale, and was able to verify the results. In that process I had developed a method in which some patients could improve their health, and a small number might be able to cure it with the right type and level of exercise. I was also recommended that exercise testing be used as a reliable scientific method of diagnosing CFS. I knew that sooner or later, someone else would use the abnormal response to exercise as a diagnostic method and copy it, or develop it independently, but I am the originator of that method. I was also the first person to describe the abnormal delay in recovery from excess levels of exercise which is now called “post -exertion malaise”. An example of someone claiming to have invented that as a “new” idea 38 years later (now, in 2013) can be seen below. Of course, I wish him luck with this research, because it will be of great benefit to chronic fatigue patients who have a real, physical ailment, but it would be nice (and ethical), if someone would admit where all of those good ideas came from – me. Ripon, CA. August 8, 2013 – Workwell Foundation announces the publication of a new study supporting previous findings that a 2-day Cardiopulmonary Exercise Test (CPET) protocol objectively documents post-exertional malaise (PEM), the most commonly recognized symptom in Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (CFS/ME). The study revealed a statistically significant performance decrease on Day 2 in workload at ventilatory threshold (VTWL), workload at peak exercise (WLpeak), volume of oxygen consumed at ventilatory threshold (VTO2) and volume of oxygen consumed at peak exercise (VO2peak). In short, individuals with CFS/ME were unable to reproduce their Day 1 performance on Day 2. The statistical classification analysis points to a diagnostic biomarker for CFS/ME with a 95.1% accuracy. Who Benefits? My comment. The only reason such methods are being reported as “New” is because no-one is acknowledging my research, and the only reason that qualitative diagnosis have been used rather than scientifically objective methods for the past few decades, is because my methods have been ignored. Patients have been given wrong advice for decades, and have been denied their entitlement to insurance etc, because my research has been ignored. See here. |
The PACE trial of 2012 used my 1982 principles
Max Banfield at about the time I started researchWhen I walked out onto an oval to treat my own chronic fatigue in 1976, I didn’t know that I was the first person in the world to do it voluntarily. Nobody could tell me how to do it, so I had to develop my own methods. Since then other people have called that method “Graded Exercise Therapy” with the specification that the person trains within their own limits. Nowadays it is widely regarded as the best, and most effective method of treatment. The 1982 research project was so successful that the first twelve week program proceeded into a second, and then a third study involving more than 60 patients, and I was invited to continue and extend it to 200, but declined. My method of getting the patients to train within their own limits and at their own pace has been used by many researchers since, because, if they run any faster than that they will experience the type of symptoms that make them stop training, and then it simply won’t be possible to do get any benefits, or to do the research required. None of the patients in my 1982 study reported any problems because they were told how to avoid them before they started training. However, a recent 2012 paper reports on the PACE trial of 650 patients where there were some patients reporting problems – which would relate to them being required to exercise at a higher level, or improving at a faster rate than was possible.. See the results of the four year PACE trial between November 28th 2008 and 2012 here. This is a quote from that report . . . “The treatment manuals are available, free of charge, on the Trial Information page for downloading, so long as no changes are made to the manuals. Any use of these manuals should acknowledge the PACE trial (www.pacetrial.org)“ However the authors of the PACE trial are using my methods, so they have an ethical and legal obligation to attribute those methods to me because i am the person who developed, defined, scientifically proved, and refined them. The labels of GET, Pacing, and CBT are simply the rewording and labeling of the methods which I invented. Anonymous Wikipedia editors are stealing my intellectual property by copying my methodsThis is a quote from my research paper of 1983 which describes some of information which I gave to the instructor about how to apply the exercise principles which I developed.
This is a quote from Wikipedia where a small group of anonymous editors has criticised me and my methods but then copied them in their page called “Chronic Fatigue Syndrome Treatment”, in several areas, but in particular, in the section called “Pacing” . . . “Pacing techniques encourage behavioural change, but unlike cognitive behavioural therapy, acknowledges the typical patient fluctuations in symptom severity and delayed exercise recovery.[30] Patients are advised to set manageable daily activity/exercise goals and balance their activity and rest to avoid possible over-doing which may worsen their symptoms. Those that are able to function within their individual limits may then try to gradually increase activity and exercise levels (GET) while maintaining pacing methods. The goal is to increase over time the level of routine functioning of the individual.[27] A small randomised controlled trial concluded pacing with GET had statistically better results than relaxation/flexibility therapy.[30][31] A 2008 patient survey by Action for ME found pacing to be the most helpful treatment[18] and a 2009 survey of two Norwegian patient organizations (ME-association and MENiN) had found that 96% evaluated pacing as useful.[24]” (end of quote). See here. |

What is the chronic fatigue syndrome
The word syndrome means “a set of symptoms occurring in the same patient“, and the chronic fatigue syndrome includes chronic persistent or recurring tiredness, and physical fatigue involving a reduced capacity for exertion and an abnormal response to exercise, particularly high levels of exertion.
Those basic symptoms are combined with an occasionally sense of faintness, which are all due to the abnormal tendency for the blood to pool in the lower part of the body instead of being distributed evenly to the upper part, and particularly the brain. Another characteristic symptom is a very specific form of breathlessness which is not seen in any other illness and involves an occasional feeling as if it is difficult to get a full breath, and where the patients will be seen taking one or more forced deep gasps for breath which are otherwise described as abnormal sighs.
Although there have been more than 100 different labels given for the illness, and although there have been many quite ridiculous attempts to convince the public that it is a complicated problem, and a “a disease by exclusion” (which means that after every other illness is considered it is the only one left), nevertheless, exactly the same basic set of symptoms are seen in the chronic fatigue syndrome, myalgic encephalomyelitis, Orthostatic intolerance, Da Costa’s syndrome, the Effort syndrome, Costochondritis, and many more.
People who are trying to convince the public that all of those problems are completely different have either not studied the history of research properly or are, for one reason or another, telling the public lies. e.g. see here.
Banfield’s Axiom for the Chronic Fatigue SyndromeAn axiom is a self-evident truth, or a statement which is so obvious that it can be taken for granted without any need for further scientific proof. “Chronic fatigue syndrome is a physical ailment where many patients have benefited from appropriately designed exercise programs because it is a physical illness which has responded to a physical treatment method”. © |
Many patients with chronic fatigue are now being treated with the appropriate exercise training, within the individuals limits, and the lifestyle modifications which I defined in 1982. Those principles have become the basic templates for all exercise treatments for chronic fatigue since, including PACING and Graded Exercise Therapy. See here.
Methods of diagnosis
The main feature which distinguishes the various types of chronic fatigue syndrome from normal health is the abnormal physical and physiological response to physical exertion.
Therefore, where that feature exists, it doesn’t matter what label is used, it is still the main feature, of the main type of chronic fatigue syndrome. See here
The methods of diagnosis which I recommended in 1976-82 were exercise testing here and here, and graphs and measurements and all wired up and aerobic capacity and tilt table tests here, and more recently the DATT method.
See a modern report on diagnosis provided by Tom Kindlon on Twitter on 12-10-13 here.
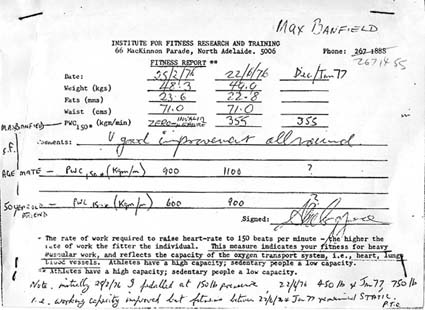
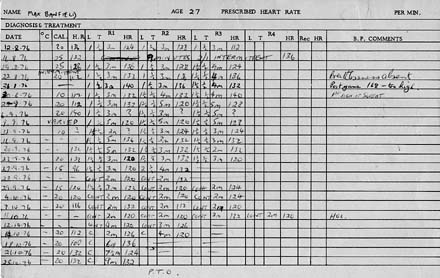
Why I was invited to sign the chronic fatigue research programSee my full report here. In 1976 I had various health problems which were not responding to treatment so I decided to attend standard exercise classes at the South Australian Institute for Fitness Research and Training in an attempt to gain some improvement. Upon enrolment each person was required to ride a stationary cycle for three minutes while their chest was attached to wires which led to a cardiograph machine. They then rested for three minutes and repeated the process up to seven times, where slight pressure was added to the brake each time. Research cardiologists then produced graphs to determine fitness levels. The scan below is a report which shows that my level at 25-2-76 was zero. I was later told that it was invalid because most graphs are straight line measurements, but when it is as low as mine a curve should be drawn, and that my actual level was between +10 and 100. I trained twice a week for 12 weeks and was retested with a result of 355, as can be seen in the report below which was signed by one of the research cardiologists. I continued and increased my frequency gradually until I was training 3 times in groups at IFRT venues, and 3 times on my own at local ovals, and I improved from slow walking to slow and intermittent walking and jogging. I was retested in December/January, but despite my improved levels of exercise, my measurable aerobic capacity remained at 355, so I added it to this report in my own handwriting. (note that the report below was given to me after the second medical examination and it included the results of the first with the comment ‘ V (very) good improvement’. The next test was taken several months later. I don’t recall being given a copy of the third result but I was told the measurement so, somebody, perhaps myself, added it to the next colum) I also added some notes about a friend of mine who was the same age, and who started at 900 and after 12 weeks was 1100, and a 50 year old man who I met told me that he had improved from 600 to 900. I was also told that an average sedentary worker would give a measurement of 700 and an athlete 1200. The institutes report can be seen in the first scan below, which includes my notes. Each person was also given a card to record the dates on which they trained, and pulse rates, so I have scanned a copy of the period 12th August to 5th October, which shows that I trained on the 20th, 23rd, 27th, 28th, and 29th of September 1976 (five times in that 10 day time span). See below. Seven years later I explained what I had done to the head of the Institute and he invited me to design and co-ordinate an exercise program specifically for patients who had chronic fatigue. See here and the test results from that study here.
The following quote is typical of general opinion before I started that program . . . In 1974 J.W. Hurst wrote a reference book which included this topic and had these words . . . “the patients could not or would not follow the prescribed training programme”. The most widely accepted view was that such patients had never played sport in their lives, and were refusing to train because they were afraid of the “normal” symptoms oijiuf exercise. See more here. In fact, I had played sport for up to 7 days a week for many years, and conducted exercise sessions regularly, and probably had more practical experience with the response to exercise than 99% of the population. See more here. |
The category of “Standard” chronic fatigue syndrome(Where the only features are the physical symptoms)There have been many disputes about the cause and nature of chronic fatigue syndrome and more than 100 different labels, so I will present the category of “Standard CFS”. It involves the relevant physical symptoms and none of the psychological aspects. It is the basic and uncomplicated type where the main features are an abnormal response to exertion, and the associated physical symptoms, but where there is no evidence of anxiety, depression, or any other psychological disturbance outside of that which is generally seen in healthy individuals. In that regard the term “diagnosis by exclusion” applies. Such a category should apply to all undetectable illness, or any illness where the cause is a matter of speculation or dispute. |
it doesn’t matter if the chronic fatigue syndrome is caused by anxiety, a virus, or poor posture, or whether it is genetic and the person is born with it, because after it has been acquired it is a physical condition, and anyone who argues against that fact is wasting their time because there is already a massive amount of scientific evidence to prove it, and more will come in the future. Diagnosis and treatment needs to be based on that fact.
I started arguing against people who argued that it was a psychological disorder 35 years ago and I have been winning since day 1.
The dilemma that all chronic fatigue patients have to face
A dilemma is a situation in which there are only two choices and neither is going to solve the problem properly
Chronic fatigue syndrome is a real physical ailment which involves real physical limitations that indicate a reduced capacity for the normal activities of life. However unscrupulous researchers shed doubt on that scientifically proven fact and argue that it is an undetectable, and therefore mental illness.
This leaves the patient in a position where they have to follow the basic principle of choosing the lesser of two evils.
Namely, they restrict their activities, in which case they are labeled as lazy or mentally ill. Their second choice is to try to keep up the pace of a normal lifestyle and soon become exhausted to the extent that they can’t do anything even if they want to, in which case the are going to be labeled as faking illness.
The dilemma is that it doesn’t matter what choice they make because they are either going to be labeled as lazy or mentally ill . . . or . . . faking or mentally ill.
The best thing to do in that situation is to stay within limits and remain reasonably healthy all the time, and just avoid, ignore, or tolerate the criticism.
When Pavlov’s dogs were experimentally placed in situations where they had to distinguish between circles and slightly oval shapes to get a reward, they became frustrated and went mad, and the same thing happens to humans. Some unscrupulous researchers will then say . . . “look, we told you so, the patient is mentally disturbed, which proves that mental illness is causing the fatigue”.
The big picture, and the patients big problemFor the past hundred and fifty years many patients with chronic fatigue have been told that they are just “whinging” about normal tiredness, or that they are “imagining” that they have abnormal fatigue, or that they are just “lazy” or that they are just complaining about the type of normal fatigue that normal people would not fuss about, or that they their health problems have a psychological, and not a physical basis, and that their illness is mental and not physical, and that all they need to do is stop worrying and their symptoms will miraculously disappear. During the same 150 years the microscope and X-rays, and other advances in diagnostic technology, have been developed, and or, used as ways of diagnosing illness, and have demonstrated and proven that there is a real physical basis for some types of fatigue. The patients who were previously misdiagnosed as having a mental illness have expressed great relief that the real cause has been found, and that they are no longer worried or depressed by the suggestion that they were just mental cases complaining about nothing like “all” of the other patients whose illness was undetectable. In the meantime “all” of the other patients still have to deal with the accusations that they are just mental cases whinging about nothing. The element of doubt still exists, and the onus of proof continues to be placed on the “victim” of the illness’s. The best way to resolve this problem is for “all” people with chronic fatigue to be “united” as “one”, and “stick together”, so that whenever a scientific method is developed to prove that a particular group of patients have a “real” “physical” ailment, then “all” patients have a real illness, which is not recognised because the diagnostic technology to prove it is not yet available. In that case the “element of doubt” will be placed squarely on all of those people who argue that the illness is trivial or imaginary, and the “onus of proof” will be on them to prove their “argument”, instead of the patient. If patients don’t unite in this manner, then absolutely nothing will change in the next 100 or 1000 years and they will continue to have exactly the same problem with their credibility. |
Diagnostic Tests
My research method is a way of easily diagnosing CFS here.
See another way of easily and scientifically diagnosing the physical nature of the illness with tilt table tests. See here, and here, and here.
Comprehensive treatment for CFS
Many diseases have multiple causes, and require multiple methods to produce the most effective treatment, and that applies to the Chronic Fatigue Syndrome.
In my case I avoid situations which involve poor posture. I also have a healthy diet, and do a lot more exercise than most people, but always within my limits, so it mainly includes walking, and I don’t hurry or worry. I also lead a lifestyle which is moderate and avoids any undue demands on my time, or requires persistent or prolonged activity which is likely to have adverse effects, and participate in less demanding activities, which from trial and error experience, don’t cause problems.
How do you stay within your changing limits
Some people enquire about how to determine their limits and stay within them. It is not a matter of being mathematically precise but of knowing your approximate range of limits, and taking into account that they will often vary by some degree from day to day, and adjusting the limits accordingly. The easiest way to do that is to constantly stay below the level which is likely to cause fatigue. It is not as difficult as it seems because it is like driving a car where the speed limit is 60km per hour. If you are constantly driving at that speed you are likely to exceed it from time to time, but if you constantly drive at that level or lower you are unlikely to be booked for speeding.
Biographical science and mathematical science
When I began studying my own health problems in 1975 it was obvious to me that my own doctor didn’t understand them, and couldn’t explain them, and it soon became apparent to me that many of the world’s top researchers had based their ideas on reasonable but wrong assumptions. Others had dismissed the symptoms as trivial or imaginary, and were not doing any useful research at all, so if I didn’t do something to change the situation they would probably never solve the problem, at least not in my lifetime
I studied the symptoms myself by recording very detailed observations, and later described them in essays and submitted them to such places as the Australasian Nurses Journal for publication.
For example, one of the most popular ideas was that the symptom of breathlessness was due to anxiety, so I described how tight belts, tight shirts, and leaning toward a desk were compressing my lungs and restricting my breathing and contributing to the problem. That essay was called “To breath or not to breath – is that the question” and it was published in May 1978 page 5-6.
I considered that other researchers would then be able to start with a correct understanding, and find mathematical laboratory observations, and do x-ray and CAT scan studies which were equally as accurate, and which confirmed the correctness of my “biographical” science. (mathematical science and laboratory science would match biographical science).
There was also the general idea that the patients were unwilling to exercise because they were afraid of the normal symptoms of effort, and that it stemmed from the fact that they had never played sport, so they didn’t know the difference. However, I had played sport, and I did know that they were different, so I described them in great detail. I also researched and scientifically proved some of those differences myself, at the South Australasian Institute for Fitness Research and Training. See here.
Nevertheless some people have been trying to hinder the research, and shed doubt on it, and create confusion, or hide evidencet, and in that process would like the public to believe that I am an insignificant kook who is a mentally ill hypochondriac with an obsessive compulsive anxiety disorder and a morbid preoccupations with the trivial details of illness.
Their interpretation is ridiculous.
The economics and politics of research
Ever since World War 1 the military, governments, and major corporations have known that a person who develops chronic fatigue at the age of 20 will still have the problem at 60, and will eventually die of old age like everyone else.
They have known that it is a physical problem of some sort, and that there is no cure, and that each of the more than 50,000 soldiers who had the ailment in 1919 was entitled to financial support and compensation for the next 40 or more years of disability and unemployment amounting to trillions of dollars per year. However they don’t want to make those payments, so they have been doing everything possible to ignore, discredit, or hide the scientific proof of physical cause, and funding research programs to invent arguments that it is a mental illness involving trivial, imaginary, or fake symptoms which will cure by themselves with a few months or years of rest. They have therefore been able to avoid the trillions of dollars in expense.
Their arguments have included the idea that you can trust their own researchers because they are highly qualified, but you can’t trust what patients say because their self-reports aren’t reliable, and you can’t trust the research studies which haven’t been accepted in journals, and that even if proof is provided it can’t be trusted unless many different researchers verified the same results in several different reliable sources.
Essentially they have been inventing all sorts of excuses for not accepting the obvious fact that millions of people have the chronic fatigue syndrome, and that they are all entitled to compensation, and that the vast majority of them have been denied their genuine entitlements for the sole purpose of saving corporations, the military, and governments the expense.
Patients with chronic fatigue syndrome have an incurable ailment which is regarded by many people as a financial burden to society which it is not prepared top bare, so it funds the “all in the mind” theories to make it “disappear”along with the responsibility for it in a manner that applies to most other illnesses. See here.
The changes in attitude since my research project
When I started a research project in the early 1980’s there was the popular view that the symptom of abnormal fatigue was trivial, imaginary, or was due to laziness, or lack of exercise, or the fear of exercise, or anxiety, or just excessive concern about the normal symptoms of fatigue.
By the time the project was completed I knew that I had scientifically proven that they symptoms were real and physical.
I therefore knew that there would have to be a major change in attitude toward the problem, but I didn’t know how that would happen.
However, as years went by, I became aware that the label of Da Costa’s syndrome (where the main symptom is fatigue) went into disuse, and was replaced by the more common use of the label of the “Chronic fatigue syndrome”.
It has also become obvious to me that a lot of people resent the fact that a patient made this discovery, and that they don’t want to acknowledge that my research was responsible for the change in labeling. They don’t even want the rest of the world to know that I exist, and they argue that Da Costa’s syndrome is not even related to the chronic fatigue syndrome. e.g. See here.
You can read my research project below, and judge for yourself. My critics don’t want you to read or know anything, but just to thoughtlessly assume that the changes came about for some gradual or obscure reason.
The Research Project
South Australian Institute For Fitness Research And Training (1982-1983)
Study co-ordinator: M.A.Banfield
The South Australian Institute for Fitness Research and Training was based in MacKinnon Parade North Adelaide in a two story building with an outside quadrangle for exercise. The ground floor consisted of change rooms, etc, and the top floor housed the reception area, office, and managers rooms, and the medical examination room for patients and diagnostic equipment such as ergometric cycles and cardiographs. The building was across the road from the University of Adelaide sports ground which was also used as an exercise park. The Institute also had venues at the Magil (Teachers College) campus of the South Australiaian College of Advanced Education, and the St.Bernard’s Recreation Centre, which was a large basketball stadium in the northern eastern suburbs. They had been conducting research programmes to assess the effects of exercise for several years on thousands of patients before I became involved and had programmes specifically designed for the general public and for people with obesity, asthma, arthritis, and heart disease etc.
I first participated in the programme for the general public in 1975 and later designed a programme for people with chronic fatigue starting in 1982.
In order to run such a programme which involved human volunteers the design had to meet the requirements of ethics that met government and University science standards.
I told the head of the Institute that I didn’t wish to organise the study because I wasn’t medically qualified, but when he asked his cardiologists if they would do it they told him that they were too busy on other projects, so he persuaded me to do it myself. In order to meet the ethics standards I was required to establish a committee of six which consisted of the appropriate medically qualified members. That was achieved by the head of the Institute being part of it, and he arranged for one of the cardiologists to be on the committee, and there was myself which made three. He gave me the name of some medically qualified professionals who were interested in doing research and asked me to phone them and ask them if they were interested. Two of them were, with one being a general practitioner, and the other being a psychiatrist. The sixth member was chosen for the task of being field coach because of his extensive experience in previous fitness research programmes, and his appreciation of the different requirements that were determined by which type of ailment was being studied and treated. The programme also had to get official support so I was given the name of a politician to contact, and was required to give him an outline of the programme etc. He provided a token payment to signify that approval. The costs of the course were paid by each volunteer, but because it was officially approved, they were reimbursed the full amount by the government medical fund of that time. One of the later meetings was also attended by a medical journalist from the Adelaide “News” which was the main evening newspaper covering all of South Australia. That journalist had been kept up-to-date with developments for about two years, and wrote the newspaper articles that were the prime source of volunteers. Other volunteers responded to letters sent to general practitioners who were asked the inform the relevant patients of the course.
The objectives of the programme;
To determine the physical fitness levels of patients with persistent fatigue, and whether or not it was possible to design a fitness programme which was acceptable to such patients, and then to determine the effect of such training on fitness levels. The objective was also to compare the fitness levels of patients with persistent fatigue with that of healthy individuals.
The factor which motivated me to run this project was the research literature which indicated that most, if not all previous programmes were unsuccessful in retaining participants for long enough to get meaningful results. The general view was that “such patients could not or would not train”.
I had participated in such a course for nine months five years earlier, and was therefore confident that I could design a programme which would be acceptable to other people with similar problems.
During that time part of the training involved walking or jogging around a 400 metre oval. In general terms I would be jogging 50 yards behind the tailenders as the front runners were overtaking me. The other participants were simply trying to improve their fitness, or were exercising as a treatment for obesity, asthma, arthritis, or heart disease. On one occasion, as two fifty year old men were out lapping me, one turned to the other and said loudly enough for me to hear “that is typical of the youth of today: they are unfit because they are too lazy to exercise”. Those men did not know that I had been a gymnastics instructor for five years, and they both seemed to me to be training to treat smoking induced lung or heart problems.
I had to take those things into consideration because many people would drop out of a course due to the humiliation of coming last, and the ridicule associated with it.
I also considered that most training courses had instructors enthusiastically encouraging participants to constantly improve their training levels from week to week, and that such an approach would prompt fatigued patients to exceed their limits and start experiencing the types of distressing symptoms which would make them drop out of the course immediately.
Therefore I established the following protocols for the course.
Firstly, people with persistent fatigue would need to train in an entirely separate group, so that they all had a reasonable understanding of each others ailment.
The participants were to be informed that their objective was to train at their own pace of walking or jogging, and that they were to improve their pace according to the way they felt, and not because they were required to, and that the programme was not a contest or a race, but an exercise of staying in training for as long as possible, or for as long as their health continued to improve.
The participants were advised that the cause of the fatigue was not known, and that those who were running faster were to recognise the possible difficulties of those going slow and not be critical or judgmental about it, and the slower walkers or joggers were advised to ignore any negative comments from other members of the group, or outsiders, and to continue training at their own pace regardless.
At the outset the general view in the research literature was that:
There was no scientific evidence of a physical or measurable basis for persistent fatigue.
That patients who complained about persistent fatigue were complaining excessively about normal fatigue.
That such patients were reluctant to exercise because:
1. of a fear of exercise
2. they were too lazy to train
3. they had no desire or motivation to get well.
The Data from this Fitness Training programme indicated that:
80 people applied for the course and were tested as far as my recollections can determine, but data was not recorded for the last groups. Of the initial 3 groups data was compiled for 26 participants. Of those the measurements were adjusted according to age, body weight, and gender, and 15 were below average, 8 were average, and 2 were above average aerobic capacity. Although only 9 completed 3 months training, and only five completed 6 months training, that is not unusual for any group of patients. Groups of patients with asthma, obesity, or arthritis etc, had similar drop out rates.
The fact that 1 woman and 4 men with abnormally low aerobic capacity continued to train for at least 2 hours per night, twice per week, for at least 6 months is evidence that the former views were invalid. i.e. Patients with severe fatigue were motivated to regain their health, they were not afraid of exercise. and they were prepared to train in an attempt to achieve their objective.
It is interesting to note that of the nine people who trained, and continued for at least 3 months, only one started with above average fitness, and the other eight started out low, or very low, indicating that those with the most severe fatigue were the ones with the highest motivation to regain their former health.
The conclusion from the study was that there are a group of patients with persistent fatigue who have a measurable physical condition that responds favorably, to some extent, from an appropriately designed exercise programme. M.B.
The John Maddox Prize – who should be awarded it
When I began reading the medical literature to solve my own health problems in 1975 it soon became obvious that doctors did not understand the difference between normal tiredness, and the abnormal tiredness of chronic fatiguen, and that they didn’t know the difference between the normal response to exercise and the abnormal response experienced in chronic fatigue.
They also didn’t know that many different and varied factors induced and aggravated the symptoms, or that they varied from minute to minute, or day to day, or month to month etc, and that they would never know until an intelligent patient studied those aspects and described them in accurate and precise detail.
It was also obvious to me that any patient who did describe their symptoms in that manner would be diagnosed as a mentally ill hypochondriac who was morbidly preoccupied with the minor aspects of trivial illness, and that they would soon become discouraged from that process and give up before they or anyone else learnt anything useful.
I therefore decided that the best thing to do was to describe and record such information, and develop my own ideas on the cause, and how to relieve, manage, or cure the condition. When I started getting those ideas published it was apparent that anyone who saw the details would be better informed, but could also copy and use my ideas without giving me the credit.
I noticed that happening when I was providing information to a page about Da Costa’s syndrome for Wikipedia in 2008. Two editors in particular, had placed me on a watchlist and were following every detail of everything I wrote on every page, and were trying to criticise and delete every word I wrote, and all existence of me or my published articles, books, and website, and furtively using, or transferring the information to other pages in that encyclopedia. See here and here.
However, many of my essays were published in the Austalasian Nurses Journal in the late 1970’s, and I was invited to design and co-ordinate a research study into chronic fatigue and exercise in 1982 at the South Australian Institute for Fitness Research and Training here. I was able to provide scientific proof that the symptoms were physical and not mental. I then knew that it would be impossible for anyone to argue that the symptoms were “all in the mind” in the future.
By the late 1980’s I noticed news reports which announced that a brand new condition called the chronic fatigue syndrome was being investigated. It was obvious to me that it was just a new label for Da Costa’s syndrome.
I also published a book between 1993 & 2000 giving detailed descriptions of symptoms, and a website soon after, with similar information, and since I have been banned from Wikipedia in January 2009, I have been criticising my two critics and made it more than obvious that the ailment is physical despite their rigorous attempts to argue the opposite. See my report here.
More recently I have seen a report about Simon Wessely being granted the John Maddox Prize for his research into chronic fatigue and exercise which he started in 1987, only three years after I did my research.
I am not in a position to say if he gained his ideas about chronic fatigue and exercise from me, but my ideas were so important that they would have spread throughout the relevant research community of the world via the social grapevine. During that time he could have read, and followed my reports just as easily as my main Wikipedia critic did via a watchlist etc..
However,it doesn’t matter if there has been a breech of my copyright or not, because the first person to make scientific discoveries is the one who deserves the credit. See also my report on the cause and effect question here.
The John Maddox Prize awarded to Simon Wessely
See also a letter from Countess Mar to Simon Wessely here
The Lancet is one of the worlds foremost medical journals and on November the 12th 2012 it announced that psychiatrist Simon Wessely was one of the first winners of the John Maddox Prize. it is jointly funded by the journal Nature, and a non-profit organisation called Sense about Science, and the Kohn Foundation.
A report says that he began working with patients who had chronic fatigue in 1987 before it was called the chronic fatigue syndrome and that he has helped to define the condition. It also states that. . .
“Many people labeled the condition as non-existent and all in the mind of the patient, but Wessely took on the study of individuals with the CFS and documented the condition as both a physical and a neurological condition. In the process of providing research and clinical care, Professor Wessely received attacks, threats and deliberate distortion of his scientific publications. See here.
According to the Mayo clinic the main treatment is psychological counseling using cognitive behaviour to reduce anxiety and that “graded exercise therapy means exercise using a physical therapist to set up a program to gradually increase the intensity of the exercise so as not to fatigue the individual”
However, in 1975 I set about criticising the people who were saying that the problem was trivial and all in the mind.
I also described how doctors were telling patients that their chest pain was not due to heart disease, but were not convincing the patient. I found out that the chest pain was due to inflammation between the ribs, and recommended that they stop telling patients what it wasn’t, and start telling what it was, and then they would be more believable, and more effective at relieving anxiety. I also interpolated that staying within exercise limits could prevent problems, and that similarly, the patient should be instructed on methods or reducing their general lifestyle to moderate levels.
I had studied psychology and knew that changing the way a person thinks to relieve anxiety was called “cognitive behavioural therapy” so to fit in with the jargon of the time I used that term to describe that method.
I also used my own judgment to do exercise to improve my own health in 1975, and between 1982 and 1984, designed and coordinated a research program which proved it’s effectiveness in other patients, which was three years before Simon Wessely started. See my summary of newspaper reports from three years earlier here.
The amount of adversity that I have had to deal with because I actually have the ailment, and the amount of hostile ridicule and bias, prejudice and criticism that I have had to deal with from critics has been a lot more than anything that Simon Wessely has ever had to deal with. e.g. See here
The Contrast in Wikipedia
When I joined Wikipedia in 2007, and an email correspondent provided a summary of The Posture Theory. It was about my theory on the physical cause of many illnesses which had previously been said to be “all in the mind”. It was deleted for various reasons. When I then started adding to the page about Da Costa’s syndrome I included some details from my research about chronic faitgue and exercise which I did between 1982-4, but two editors argued that no-one had agreed with any of my ideas, and that there was nothing in the “real” medical literature about it, They managed to convince other editors to delete all of the information and get me banned by arguing that I was a non-notable fringey kook who’se ideas were nonsense and crap. They replaced my version of the article with one which described the condition as an anxiety disorder, and attributed it to fear by referring to “cowardice” in battle, and put it in the category of somatoform disorders which are imaginary disorders.
They knew, and often told other editors, that I had that ailment, and were appealing to prejudice by inferring that I was a mentally ill person and a coward suffering from imaginary symptoms caused by anxiety.
See the information which I added about my research into exercise and chronic fatigue here and some of their comments and reasons for deleting it here.
By contrast Wikipedia has a page on the biography of psychiatirst Simon Wessely who they say had studied the relationship between chronic fatigue and exercise from 1987 onwards, and provided evidence that chronic fatigue patients had a real illness that was not “all in the mind”. They also reported that he had been awarded the John Maddox Prize. This is a quote from another website
“The award is the inaugural John Maddox Prize and it was awarded jointly to the British psychiatrist Professor Simon Wessely for his courage in facing opposition to his views about ME and Gulf War Syndrome.” See here
See also a YouTube video on the John Maddox Prize here.
That contrast is astonishing
A quick summaryI proved that fatigue in Da Costa’s syndrome was not “all in the mind” In 1975 I had health problems which were not being relieved by treatment so I began to study medicine myself. I found that I had an ailment called Da Costa’s syndrome which had been regarded as having no physical basis, and which, throughout the previous century, psychiatrists had concluded were related to anxiety and fear and were “all in the mind” By 1984 I was able to design an exercise programme for other patients, and gain scientific measurements to determine and prove that the condition had a real physical basis. The name changed from Da Costa’s syndrome to the chronic fatigue syndrome Soon after that I noticed newspaper reports about a new disorder called the “Chronic fatigue syndrome”. The symptoms were the same, so it was just a new label for Da Costa’s syndrome Wikipedia deleted everything about my research When I added information about my research to Wikipedia in 2007 two editors described me as a non-medical, non-academic fringey kook who was just a patient who meant well but whose ideas were stupid nonsense and crap and didn’t deserve even one sentence of space, and they deleted everything about that research and myself until there was nothing for the readers to see. See here. Wikpedia reports that Simon Wessely argued that it was not “all in the mind” They also had a page about the biography of a psychiatrist named Simon Wessely who had various academic and professional qualifications, and they reported that he had developed new measurement toots, and used exercise methods (exactly the same detailed concepts which I developed), to help patients with the chronic fatigue syndrome, and that he was awarded the John Maddox Prize. The entire article is in great praise for his contributions to research. See here. Other websites report that the John Maddox Prize was given to him for his courage in relation to the controversial aspects related to his attempts to argue that the symptoms were “not” all in the mind. See here. He started his research on exercise and fatigue in 1987 (3 years after I completed mine). The Wikipedia Time Frame At 5:58 on 18th December 2007 I added information and details about my research into chronic fatigue and exercise to the page about Da Costa’s syndrome. e.g. here. At 00:54 on 29th December 2007 An editor named Gordonofcartoon deleted it here. At that time there was a page about Simon Wessely which had nothing evident or specific about his research into chronic fatigue and exercise. See here. At 7:18 on 21st October 2008 (8 months later) an editor named Sam Weller added information that Wessely had developed “new” measurement tools” for CFS, and a “new” “rehabilitation strategy” which involved “Cognitive behaviour therapy” and “Graded exercise therapy” and did “follow up studies”. here. At 2:48 on 23rd October 2008 an editor named RetroS1mone added information to Wessely’s page about his randomised trials into cognitive behaviour therapy and graded exercise therapy, and gave references as examples – refs Am J Psychiatry 1997 Mar:154(3):408-14, and Gen Hosp Psychiatry. 1997 May:19(3):185-99. He also described them as the most effective currently available. At 12:08 on 23rd October 2008 RetroS1mone added another two references to support Wessely’s, namely Price JR et al Cognitive behaviour therapy for chronic fatigue syndrome in adults, Cochrane Database System Rev. 2008 Jul 16;(3):CD001027, and M. Edmonds et al, Exercise therapy for chronic fatigue syndrome. Cochrane Database of Systematic Reviews 2004, Issue 3: Art. No.:CD003200. See here. At 12:29 on 23rd October 2008 RetroS1mone added the following reference – Wessely S. The measurement of fatigue and chronic fatigue syndrome. J R Soc Med. 1992 Apr;85(4):L189-90 here. At 12:41 on 23rd October 2008 RetroS1mone added comments that Wessely’s work, combined with others enable Gulf War veterans to get pensions by establishing that their ailments were the result of their service in the Gulf war and he gave the following reference http://www.newscientist.com/article.ns?id=dn6609 New Scientist] US in U-turn over Gulf war syndrome. November 3, 2004. Note that I did my initial research into chronic fatigue and exercise between 1975 and 1984, and recommended that doctors give patients useful information about their aliment (which is called Cognitive behavioural therapy). I also identified that they had physical limitations, but could do some exercise within their own limits to gradually gain some improvement, which would be useful, although it might not completely cure the problem. My research results were referred to in many newspaper reports between 1983 and 1984. Simon Wessely is described as starting his research on this topic three years later, in 1987 and his research papers were published in April 1992, and March and May 1997 (much later). ******* I added information about my research to Wikipedia in December 2007, and 2 editors described it as stupid nonsense and crap. RetroS1mone added virtually the same details about Simon Wessely’s research in October 2008 (eight months later) and called it the best methods currently available together with praise about his character and his awards. They have effectively defamed my character and erased me from Wikipedia, and put Simon Wessely on a pedestal for doing exactly the same thing??? They obviously don’t want their readers or the public to know the truth. See here. |
Death threats and character assassination in controversial research
Simon Wessely reported that death threats were made against him about his research into chronic fatigue and exercise, however, it is an obvious area of controversy, and many people have been involved in character assassination to discredit my research into the same aspect. e.g. See reports about death threats against Wessely here and here, and criticism of my ideas here and here and here.
My 1984 research paper can be seen here.
Harmful effects reported from patients in Wessely’s graded exercise programs?
Note that my exercise plan included the principle that some patients may not be able to exercise, and should not be forced to do so, and that others may not be able to return to full health, but should try to improve their fitness by gradually increasing their fitness levels. However, I specified that they should only do so by staying within their limits. and Wessely’s virtually copied that idea with different wording, but it is quite likely that not all of his instructors would have understood the importance of that aspect, or may have been overly enthusiastic about getting quick results, rather than proceeding in the appropriate manner.
Also, I knew about the adverse effects of exceeding limits from personal experience, but Wessely may have had his doubts and arranged for some of his patients to be asked to ignore their symptoms to see what happened and confirm it for himself. High drop out rates, and the harmful effects in such circumstances are typically blamed on the patient.
See my report on the harmful effects graded exercise training and how to prevent it here
See a recent list of patients reporting the harmful affects of gradual exercise training programs where some say that their instructors told them to ignore their symptoms and keep increasing their levels of exercise regardless. The list was presented by Tom Kindlon in early January 2013 and can be seen here. See another article by the same author on the website of the Bulletin of the IACFS/ME here.
Another report on the harmful effects can be seen here.
See also a page about Graded Exercise Therapy in Wikipedia, which clearly states my methods, but doesn’t acknowledge me as the source, and refers to the harmful results in some cases, without mentioning my methods of preventing those problems here.
Other reasons why patients object to Wessely’s attitude and research
The following quote comes from a criticism by professor Malcolm Hooper about Wessely getting the John Maddox Prize.
“Psychiatrists of the “Wessely School” are lead advisors on “CFS/ME” to Government Departments and agencies of State. According to them, “CFS/ME” is a “functional somatic syndrome” (i.e. a behavioural disorder) in which medically unexplained fatigue is perpetuated by inappropriate illness beliefs, pervasive inactivity, membership of a self-help group and being in receipt of disability benefits (2). They assert that there are no physical signs of disease and there is no pathology causing the patients’ symptoms, and that patients are merely “hypervigilant” to “normal bodily sensations” (3). They insist that CFS/ME should be managed by behavioural interventions including “cognitive re-structuring” (ie. brain washing) and graded exercise therapy to “reverse” patients’ “mis-perceptions”. (end of quote) here
Such ridiculous dismissive nonsense and lies have been said about chronic fatigue patients by some researchers for over 100 years. Such offensive attitudes toward patients would be causing a lot more harm to people who already have a lot of problems.
Why there are cover ups and denials about the true nature and extent of the chronic fatigue syndrome
The following words are quoted from an article by Simon Wessely about chronic fatigue syndrome . . .
“Fatigue remains as elusive a human experience as ever. At the turn of the century fatigue was almost an obsession of doctors, scientists, writers and even politicians. The scientists believed they could measure it, the doctors they could treat it, the writers describe it, and the politicians prevent it’. Many confidently expected that fatigue could be eliminated from schools, factories, armies, and even society. That it had to be dealt with was not in doubt, since many authorities believed that if not checked, fatigue, the inevitable consequence of modern life in all its forms, would somehow destroy the nation’s health and its future. Perhaps only the writers achieved their objective2 . . . The inevitable result of this extraordinary interest in all things fatiguing was a reaction, as a sense of disillusionment set in. Scientists couldn’t measure it3, doctors couldn’t cure it4 and politicians couldn’t prevent it’. Fatigue illnesses, once the backbone of any self-respecting medical text, disappeared from the indexes5. Fatigue laboratories closed6, and interest dwindled.” (end of quote)
Reference: Simon Wessely (April 1992) “The measurement of fatigue in chronic fatigue syndrome“, Journal of the Royal Society of Medicine Volume 85 p.189-190.See here.
Note that although the article is called “The measurement of fatigue”. it actually only presents evidence that it couldn’t be measured.
It also gives my readers some indication of the predicament that I was in as a patient in 1975. Namely, nobody could understand it, diagnose it, or treat it properly, so I had to do it myself. Note also that i had to use old books, and old indexes to find some of the information which is not available in modern books.
The evidence also indicates that many people at the highest level of society are trying to erase the evidence, hide it, and deny it’s existence as a real physical ailment.
See also my report on how two unethical, unscrupulous, deceitful and anonymous Wikipedia editors are trying to hide the research history of chronic fatigue from the readers here and here.
A former name for the chronic fatigue syndrome was Da Costa’s syndrome. This is what one of my two Wikipedia critics said . . .
“It is “a vague 19th century syndrome, generally considered a psychosomatic anxiety disorder). It’s overall an unimportant article for Wikipedia, so we can’t justify investing several editors’ time and energy into turning it into a little gem of an article” (end of quote) here.
See how they also tried to argue that it was a rare condition here.
See more realistic ideas about how common chronic fatigue is in the community here.
Simon Wessely Knighted for his medical and CFS research?
(Note that my father, Allan Frank Banfield, was a president of the Edwardstown branch of the Australian Returned Servicemen’s League).
On 29th December 2012 it was announced that Simon Wessely had been knighted in the New Yeas Honour List for 2013, for his contributions to medicine in relation to the mental health of military personnel. See here and here.
Various other reports say that he has developed “new” measurements for CFS, and cognitive behavioural therapy methods, and graded exercise therapy, and has been helping veterans with post-war syndromes.
See my essay on the history of medicine which includes post war syndrome here.
He is also a psychiatrist and a member of the profession which created the “all in the mind” concept, and it has been reported that he has been interested in “medically unexplained symptoms” such as the chronic fatigue syndrome and myalgic encephalomyelitis, and arguing that their illness is “not” all in the mind. e.g. See here.
He is being given the credit for my research e.g See here and here.
I have been researching Da Costa’s syndrome, which has many causes. It occurs in children and is more common in women than men, and is also called the chronic fatigue syndrome. In military situations it has been interpreted as a post-war syndrome. I have developed the concepts of limiting exercise (and gradual improvement), and adjusting and limiting lifestyle (cognitive behavioural therapy), and I have been proving that undetectable illness is real and not imaginary, which can all be seen in my ebook called “The Posture Theory”. The sub-title is “The physical basis of undetectable illness“, and it covers a wide range of causes, illnesses, and concepts. here. See more details here.
|
Some of my research One of the problems I had as a patient in 1975 was that my doctor told me that there was no evidence of disease on blood tests or x-rays, or any other scienfitcally based medical test known to medical science. Others argued that therefore there was nothing physically wrong with me, and that therefore the problem was “all in the mind” etc., and I had been called a hypochondriac. I knew that the symptoms had a physical basis and started studying the medical literature, and was soon developing my own ideas about cause, and developing effective methods of treatment. Seven years later, in 1982, the head of the South Australian Institute for Fitness Research and Training invited me to design and then co-ordinate a fitness program for other patients who had the same problems with fatigue. The first twelve week program achieved good results so it was repeated a second and third time, and then I left. In the meantime a medical journalist had been reporting the success in newspaper articles as a way of getting new volunteers into the program. I had ultimately confirmed that the ailment had a physical basis and scientifically proven that it was NOT “all in the mind”. Simon Wessely, a London psychiatrists, says that his interest in undetectable illness and cfs began in 1987, and has been given a knighthood for his research into chronic fatigue and exercise, and for helping people by getting rid of the “all in the mind stigma”??? He is taking the credit for my ideas and research. See my criticism of the “all in the mind” ideas here |
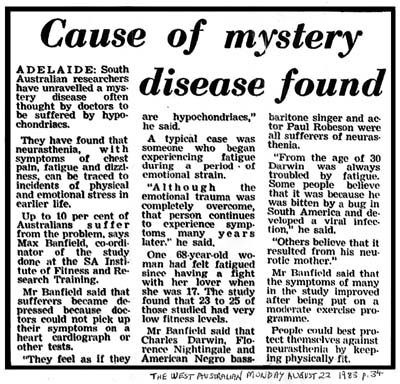
A newspaper report dated 22nd August 1983, four years before Simon Wessely began his research.
Note that I mentioned many different causes of chronic fatigue, including viral infections, genetics, and physique, etc, but the journalist chose to use one of the emotional factors, which distorts the results of my study out of proportion. See more reports here and here and here And my actual research paper here and a more thorough view the many causes here. |
|
The change in attitudes to chronic fatigue began in 1982, not 1987 My 1982-4 research project influenced world attitudes in a major way, and changed the emphasis from mental disorder to physical disorder via the label “the chronic fatigue syndrome” but the following statement is from another website called The Scientist, and does not mention it, but says this instead . . . “Simon Wessely, a professor of psychological medicine at Kings College London, became one of the first winners due to his research and treatment of hundreds of patients with chronic fatigue syndrome. . . . Professor Wessely began working with individuals with chronic fatigue in 1987 before Americans coined the term.” See here. It has been evident that some doctors are embarassed by the fact that a patient brought about this change, and that some of them have been trying to create the impression that it was due to someone within their profession. |
|
Why Simon Wessely and others had to copy my methods When I read that other researchers were not able to get chronic fatigue patients to exercise consistently I knew the reason. They were assuming that the problem was just mental, or due to a lack of fitness, and that all the patient had to do was exercise regularly, in the normal way, at progressively increasing pace, until they gradually achieved normal fitness and normal health. In order to solve that problem I designed the program so that patients could exercise within their own limits, and progress at their own rate, and continue if it was possible, or slow down, or stop if they needed to. I predicted that some people wouldn’t train, some would start and stop, and some would continue, and that is exactly what happened. Some of them did train, and improve their fitness levels, and scientific information, and a better understanding of the ailments was achieved. I also knew that it would be impossible for any other style of training to succeed, and that anyone who wanted success would have to copy my method in the future. That is exactly what Simon Wessely did, but he hasn’t acknowledged me as the source of the idea. Some patients are very grateful to Wessely, but they should be grateful to me. One of the website reports about the John Maddox Prize being awarded to Simon Wessely presents the Mayo Clinics description of the exercise program used by Simon Wessely which states this . . . “The graded exercise therapy means exercise using a physical therapist to set up a program to gradually increase the intensity of the exercise so as not to fatigue the individual.” (end of quote) here. That quote is just a rewording of the principle which I told the instructor to use at the IFRT in 1982 here. Anyone who claims that exercise programs in CFS cause harm haven’t been doing it precisely according to my design, because such people should not have started unless they wanted to, and those who did start should have been instructed to proceed very gradually and were free to drop out of the course if they had any problems. In my 1982 project all participants were voluntary.
|
I took all the risks
In 1975 I had health problems including severe fatigue, which nobody in the world knew how to treat effectively.
I therefore decided to take responsibility for my own health instead of relying on doctors. In that process I had to take risks and use trial and error methods which sometimes resulted in mistakes which I had to learn from quickly.
About 7 years later I was asked to design an exercise program for patients with chronic fatigue which was safe, and where there was no risk of mistakes.
Simon Wessely has obviously copied my methods, but not properly, and if, in some cases, there have been harmful effects, it would be because the patients exceeded their own limits. That is Wessely’s fault, not mine
He has been given an award for courage in science because some patients have made death threats against him???
Somebody should give me a chest big enough to pin a medal on.
|
In order to conduct the research in 1982, a number of requirments were necessary to authorise the project. Official Government approval and basic funding was one of the main ones. The approval letter signed by Michael Wilson, the Minister for Recreation and Sport, can be seen below, dated 15th March 1982..
The Original 1982-84 Research Paper presented on this webpage on 17-1-2008 minor editing of the text was made on 21-1-2011 The Effects of Regular Exercise on patients with Chronic Fatigue (Neurasthenia)
Introduction: Between 1982-4 The South Australian Institute for Fitness Research and Training had undertaken two studies of the effects of regular exercise on volunteers with chronic fatigue (neurasthenia). The objectives of the programmes were to determine the fitness levels of such patients prior to training them in jogging/exercise classes twice/week and giving follow up tests at three monthly and six monthly medicals to determine their progress. The fitness level was determined by requiring each volunteer to ride a stationary cycle on which varying loads of resistance were applied to the wheel whilst, at the same time, pulse rate was being recorded. By this means it is possible to graph the amount of load in kilograms required to give a pulse rate of 150 beats per minute. This figure is a gauge to each individuals relative fitness and is known as the physical working capacity (PWC 150) We also aimed to determine the extent to which neuroticism was responsible for the fatigue by asking each applicant to complete a modified version of the Middlesex Hospital Questionnaire of Crown and Crisp. (Although this questionnaire included questions of symptoms, thus giving a higher score for this type of recruit anyway, it nevertheless provided a relative guide for neuroticism comparison.) Finally, our second study included questions aimed at elucidating the affects of the fatigue on lifestyle. Results: As the result of twenty-six medicals and questionnaires (Diag. 1), it was found that fifteen enrollees had fitness levels below average, seven were average, and two were above average. (One was not known at the outset.) There were eight examples of those with low fitness who had lower (below 30) neuroticism scores, which indicated that the fatigue may be attributable to limited aerobic capacity). There were five examples of those whose fitness was average to high who had higher neuroticism scores (above 40) indicating that stress may be the primary factor causing fatigue. Other figures were not so clear. With regard to training (Diag. 2), seven did not start, and eight did not complete three months and were not re-tested, and of the remainder, ten continued for three months. Of these ten, five continued for six months. In the first three months, three participants did not benefit from training,. A further three improved to sub-standard levels and four continued toward normal levels. Of the five individuals who persisted for six months, improvement generally continued at a lower rate. One example of a participant who originally developed neurasthenia following a coronary improved dramatically. Another individual demonstrated persistent low figures despite continued training and he is undoubtedly a true neurasthenic with impaired aerobic capacity. Four participants who did not train attended a medical after six months and demonstrated relatively static fitness levels. (Diag. 3). In a second study of twelve volunteers, we asked questions on lifestyle. Of these, eight who had to make restrictions and changes all had low to very low fitness levels. The remaining four with average or above fitness did not report a need to change lifestyle. The work of Wheeler et al. provides documented information on the varying extent to which this ailment affects patients’ lifestyle but has no correlating data to account for this. Conclusion: It appears as though there are two distinct causes of chronic fatigue. Firstly, abnormal low levels of fitness and, secondly, stress (as per neuroticism profiles). However, there were examples of individuals in whom other factors may be involved. There was further evidence that low levels of fitness are responsible for the changes or restrictions to lifestyle seen in many patients with chronic fatigue. Regular exercise improves the fitness levels of most individuals. However some, particularly those with very low fitness, do not appear to benefit from the training. The latter may have an impairment in their aerobic capacity perhaps resulting from poor diaphragm accommodation which results in low ventilatory efficiency. in exhausting work as found by Wolf, Cohen et al. In consideration of all these factors it would seem that the provision of a moderate exercise programme is worthwhile for patients with chronic fatigue because of the benefit achieved by some participants and further research in this area would be valuable in assessing cause and prognosis. Acknowledgements: Bibliography 1. Mohler,I.C., Exercise Testing in Coronary Heart Disease, Academic Press, New York, 1973, pp.13-44. 2. Volkov, V.S., Psychosomatic Interrelations and their clinical importance in patients suffering from cardiac type NCD, Sov. Med,. 1980 (11), 9-15, Eng. Abst. 3. Crown., S. and Crisp, A.R., A short clinical self-rating scale for Psychoneurotic Patients, The Middlesex Hospital Questionnaire ()M.S.Q.), British Journal of Psychiatry, 1966, 112, 917-923. 4. Wheeler E. O., et al., Neurocirculatory Asthenia (Anxiety Neurosis, Effort Syndrom), Neurasthenia), A Twenty Year Follow-Up Study of One Hundred and Sevent- Three patients,The Journal of the American Medical Association, March 25, 1950. 5. Wolf, S., Sustained contraction of the diaphragm, the mechanism of a common type of dyspnea and Precordial pain. Journal of Clinical Investigation, Vol. 26, 1947, p.1201. 6. Cohen, M.E., Johnson, R.E., Consolozio, P.C. and White, P.D., I.F.R.T. Neurasthenia Fitness Instructors’ Information Sheet Aims 1. To improve the physical working capacity of n.c.a.’s. 2. To provide information about the condition 3. To provide instructions on how to control the condition 4. To gain scientific information on the condition to aid research. Methods 1. General neurasthenic principle 2. Neurasthenia and the heart: Information
(c) If fainting occurs, and the pariticpant falls to the ground, blood flow to the brain is aided by the reduced affect of gravity and the participant wakes up. (d) Charles Darwin became neurasthenic at 30 and died at 72. Florence Nightingale neurasthenic at 30 died at 93. 3. Neurasthenic exercise principles: 4. Personal and social principles:
5. Medicals at: 1. commencement And for . . . (a) patient surveillance (b) source of research information Note: This information applies to neurasthenia. However, some recruits who experience palpitations may not necessarily be neurasthenic and therefore may respond normally to exercise and not need to be restricted in their activities. Such individuals should be encouraged to train regularly and to keep fit. |
 |
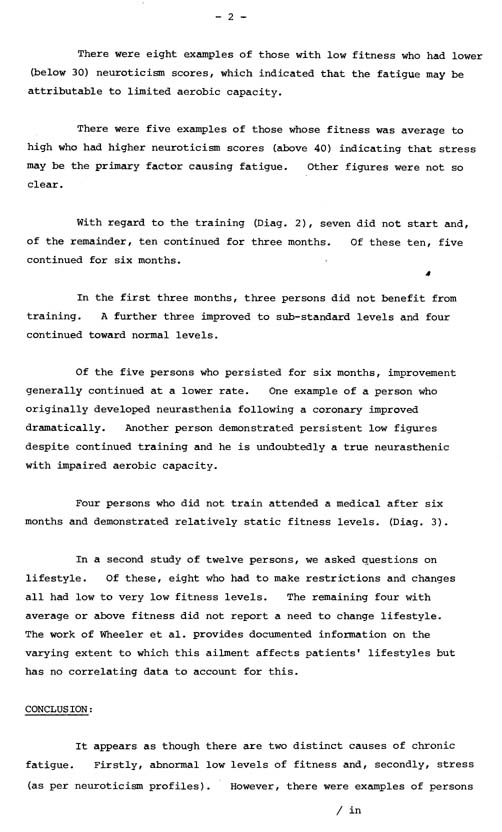 |
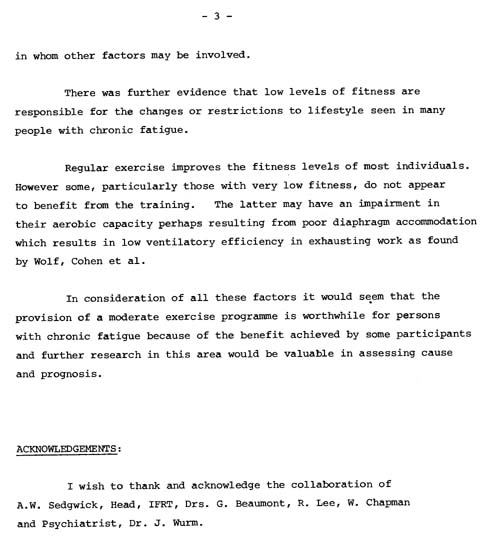 |
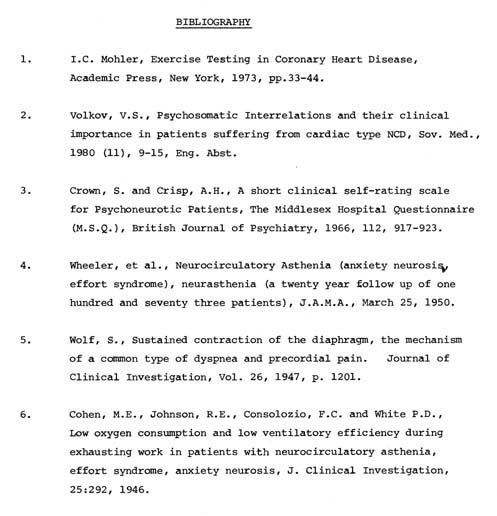 |
 |
 |
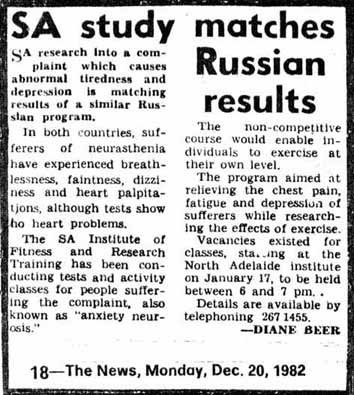 |
Copies of the original typed draft, and an earlier newspaper report comparing the study with similar Russian measurements which didn’t include the effects of exercise.
Test Results
The Aerobic Capacity (physical fitness level) of volunteers with persistent fatigue
Copies of the original graphs
|
|
See a modern report provided byJanelle Wiley on Twitter on 21-10-13 with a link to a Phoenix Rising website which evaluates the PACE trials. here. The webpage title is . . . “ME Analysis: Evaluating the results of the PACE study”‘ The PACE trials are a copy of my basic principles and the evaluation is consistant with my findings between 1976 and 1982/3. It is essentially a peer reeview of my research. However, I have determined a lot more since 1982, and know what the problems are. My study was also at the start, and after 12 weeks, and after 24 weeks of training, and the advantage I have is that I invented the method which nobody could do before, and which made all subsequent research possible, and have had 38 years more study and experience since. |
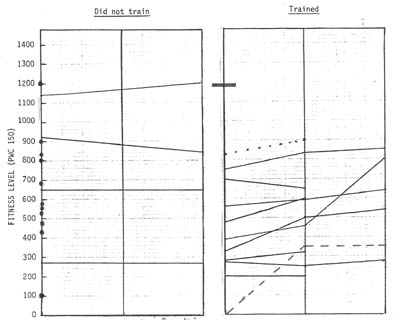

![]()
|
|
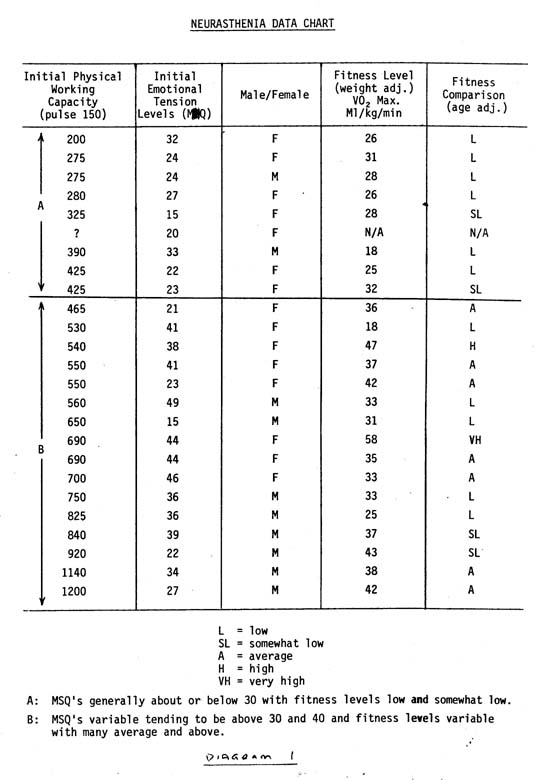
|
48 Interviews from: The Institute for Fitness Research and Training chronic fatigue study (1982-84) The chronic fatigue study also included a questionaire about symptoms and lifestyle and questions about the cause and nature of chronic fatigue from 48 interviews from about 60 phone calls, in a study of more than 200. Those interviews are summarised below. 1. After a bout of glandular fever during Matriculation exams the person never got over it. Now has tiredness, missed heartbeats, stomach pains and dizziness. 2. Started with tension in the home, and now tired all the time. Would not be depressed if it was not for the tiredness, and has headaches. Works sitting all day as a typist with difficulty and strains to read. Never had a lot of stamina. When she was a housewife she could arrange her workload to suit her energy level, but when she got a job the demands of the workload drain her energy. 3. Was a very fit person who used to go surfing, but after giving birth she had a breakdown and shock treatment, and 20 years later still gets tired and dizzy, and leads a restricted lifestyle which is a “bloody nuisance” because she can’t go out at night. 4. An alcoholic with palpitations, chest pains and tiredness who was depressed by his symptoms and reluctant to attend courses which involve social situations. 5. A university lecturer who had a family history of nervous breakdowns, and was bedridden with fatigue, first occurring after study pressure. He has been told that he is very fit on a treadmill. 6. Home stress, and work stress caused many symptoms including palpitations, breathlessness and nausea. She sees herself as just a machine in a meaningless job who is always rushing around and is put down by males, and told that everything is her fault, she gets no recognition, and has no control over her own workload due to her superiors. 7. Previously nervous but fit until the death of her husband three years earlier. She gets palpitations on waking, and is lethargic, and feels guilty about laziness and hypochondria because her doctors can’t find anything wrong with her. 8. This woman had measles during childbirth and on the day of giving birth developed palpitations, giddiness, and hyperventilation, which continued for four years, and since then she had been prone to symptoms. The symptoms caused her misery when they wouldn’t go away, and she found it hard to explain them to her husband. 9. A healthy man had been interviewed on radio when he was attempting to break a world endurance record, and was praised as a role model for today’s youth for his positive thinking, determination, and stamina. When I phoned him to enquire about his subsequent health he said that he became fatigued during the attempt, and returned to work and was still suffering from tiredness three months later when his boss told him that he was lazy and sacked him, and he had continued to be tired since. 10. This man had depression following Bell’s Palsy due to a virus in the 7th cranial nerve? 11. This person was healthy until June 1982, when she got a virus and became dizzy, fatigued, and faint, and had not recovered, and slowed down, gained weight, and complained of lethargy. 12. This person was tired, breathless, and nervous. 13. This woman’s husband caused her stress, and she had kids, and did shift work. 14. Teacher stress was the cause of fatigue 15. This person reported sudden tiredness which was inexplicable. 16. This person injured his back at home, changed jobs, and lost confidence. 17. This man was an opal miner who got Quinsy, which is a throat infection, he collapsed, and has “been useless since then” – February 83. 18. This woman described herself as a worrier, and boredom contributed to her fatigue which was “helped a lot” by a curette. 19. This woman reported that suddenly one day seven years ago she became tired for no reason, and had tried everything reasonable to cure the problem because she was in despair about her families reaction to her fatigue, and her doctors’ negative attitude about it. 20. This person exercised a lot and participated in the City to Bay Fun Run. 21. This person was on sickness benefits. 22. An 82 year old had been healthy until a long bus tour and a virus, and now is very tired, needs to rest, and is confined to a helping hand home. 23. Three years earlier the woman had her third child with extra family worries which accumulated, and then 1 year ago had tiredness, giddiness, loss of appetite, nausea, and weight loss, and found that rest in hospital, medication, and exercise helped. 24. Had problems for three years which became worse after viral pneumonia in July. 25. This elderly lady’s husband became ill, and then she was “run off her feet” with caring for his needs, and has been tired all the time in the three months since. 26. This woman said she was a tense and anxious type of person. 27. This woman was a Government Administrative Officer who developed agoraphobia since a period of work stress. 28. This woman said she had agoraphobia and couldn’t leave home without help. 29. A 65 year old man developed symptoms soon after becoming a POW (prisoner of war) in 1941 – 40 years earlier – he has had to restrict his lifestyle ever since, and eventually accepted it, and got used to it. 30. This elderly woman said she had always been nervous, and described herself as being agoraphobic for about 17 years, and the death of her husband made her symptoms worse. She suffered from dizzy spells and was “afraid to go along the street for fear of having another dizzy attack”. 31. This middle aged man had back and neck problems, and exhaustion since a car accident six years earlier. 32. This man had paroxysmal tachycardia four years ago, and since then has been tired and exhausted all the time, and said that his blood oxygen was low. 33. This man said he was agoraphobic. 34. This elderly man was too old for the fitness course, and said he had muscular fatigue, probably M.E. (myalgic encephalomyelitis). The flu made it worse, and he had an enlarged heart, and congested cardiomyopathy. 35. This man was a relieving bank manager who worked day and night, and had a nervous breakdown about a year earlier, and had been agoraphobic for about 6 months. 36. This man had been hospitalised for a few months with disabilities which may have been related to anxieties involved in his work as an assistant service manager. 37. This man reported that his symptoms came on gradually. 38. This man did weight lifting. 39. This man worked 18 hours a day, and ran 4 businesses at once, and wore out. He then gave up working 18 hours per day and expected to rejuvenate with rest, but didn’t, and continued to suffer from fatigue ever since. 40. This woman had been to the Fitness Institute courses before and was a physically fit shift worker who tired easily. 41. This woman had ventricular fibrillation thirteen years ago, and was divorced 8 years ago, and has had dizziness for 5 years. 42. This elderly woman had been harassed by her neighbour, and was awoken during the night because of the noise made by her neighbour, and had a heart murmur, and headaches due to a spinal problem, and could not attend fitness classes because she had no transport. 43. This man had narcolepsy at work, and cataplexy, and elation caused it, so he avoided elation at the first sign of symptoms. 44. This man got viruses twice per year associated with fatigue, and was always fatigued, and when he did anything a little out of the ordinary he became unduly fatigued, and was extremely annoyed that it affects his lifestyle. 45. This woman said she was short in height and overweight at 13 stone. She had suffered from fatigue since her first child kept her awake all night, every night for 9 months, and the second child did the same 14 years ago. 46. This woman started getting fatigue when she left school and started work as a nurse doing night shift. She said that she now works only 1 day per week, and is a very calm person, and that her fatigue has “nothing to do with stress”. 47. This woman enquired in relation to her son who was quiet and shy, and had asthma as a child, and became a very fit muscular man who did weight lifting, and was a canoe instructor, and played basketball. Three years ago he lost balance and became giddy and vomited, and couldn’t get out of bed for 10 days to 2 weeks because of vertigo every time he lifted his head off the pillow. He recovered after 4 weeks and has had 2 or 3 mild attacks since, and now gets dizzy, and is fatigued all the time, and is tired and in bed by 9 p.m. 48. This woman reported symptoms which she said had preceded her marriage break-up.
It is clear from this set of interviews that there are many different causes of fatigue, and many types, symptoms, and outcomes. M.B.
|
End of research paper written in 1984
More details from the 1982-4 research study
(In December 2012 I was asked to provide more information about my 1982-4 research design and methods, so I searched through my old files from thirty years ago and found the information below.)
The organisation of the study began in 1982, and the first period of training started on 17-1-1983. Each person trained twice per week on Mondays and Fridays for one hour each time, which included 20 minutes of light exercise and 20 minutes of walking or slow jogging, with the remaining time involving light recreational activities.
After the success of the first period, a second 12 week training program followed soon after.
My records show a list of 63 applicants for the project, with two late enquiries, making the total of 65. I had tried to phone each of them at that time and was able to have phone interviews with 48, which I have previously reported here.
At some stage the name of the program was changed to Project 24. It relates to the objective of having each person train for 24 weeks to determine the longer term affect of regular exercise on their aerobic capacity.
|
The program changed from research to become routine procedure I had established the pilot study and confirmed the methodology, and reconfirmed it in the second period and then left the Institute. It would then have been a routine procedure with predictable results which anyone could reproduce in the future. However, I don’t know what happened at the Institute after that in any detail, but I did learn that one of the participants continued to train, and that a few months later he participated in the City to Bay fun run, for a distance of six miles, I found copies of the project specifications and have scanned them and presented them below. It refers to a study to be continued in 1984. |
This was the description of Project 24 which I wrote, and which was typed by the Institutes typist, and presented with IFRT letterhead
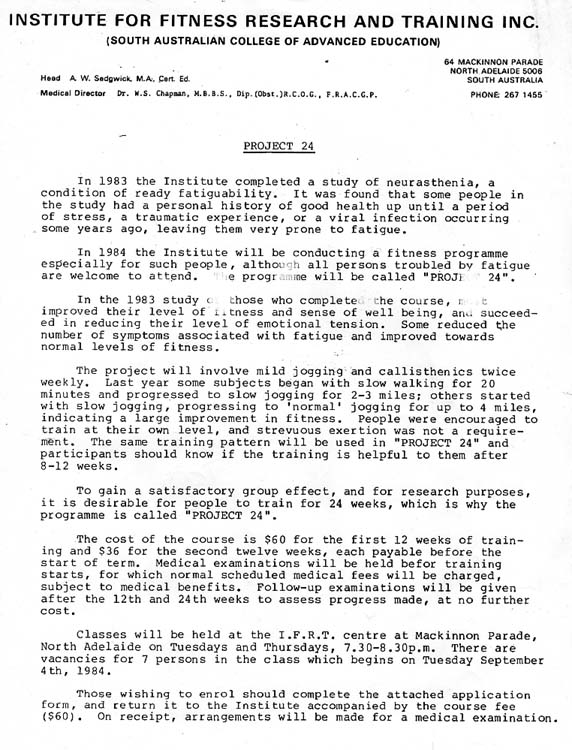
|
I described the principles, methods, and objectives for the project on two and a half pages which can be seen below . . .
Page 3
At the stage where there was data available on 65 individuals, the head of the institute, Tony Sedgewick, asked me to increase the study to 200 for the purpose of having a major influence on world opinion, but I decided not to continue for reasons which I may discuss later. In the meantime I said that the existing participants could continue to train under the same instructor, and that anyone else who wanted to continue the research could do so because the principles had been clearly identified and proven. Plagiarism, or intellectual property theft Plagiarism is “the act of using another person’s words or ideas without giving credit to that person”. “Intellectual property is “an idea, invention, or process) that derives from the work of the mind or intellect” “Peer review – a process by which something proposed (as for research or publication) is evaluated by a group of experts in the appropriate field” Reference: Merriam-Webster online dictionary here and here and here.
When someone steals a car it is a crime called theft. Similarly when someone steals an idea it the theft of their intellectual property, and is a crime called plagiarism. I have produced many ideas to treat my own health problems, when no-one else could, and my research scientifically proved several aspects. In particular that chronic fatigue involved limitations to physical capacity, and that by staying within them it was possible to exercise safely, and that by continuing to train in that manner it would be possible to gradually gain some improvement in fitness, and general health. I also established principles by which some other patients could, and did get similar benefits, and have since described them here. I have since described the type of problems I had with exercise, in particular with the characteristic breathing abnormalities which kept me within those limits here. The scientific method which was used to measure the results in my 1982 project was to have each person sit on an ergometric cycle and peddle against intermittently and progressively increasing amounts of pressure applied to the brake, while the their chests etc were attached to wires which led to cardiographs etc. The results were impossible to fake, and did establish that limits to improvement existed, and that the measurements were accurate and could be used to reliably diagnose the capacity of each individual Recently I have seen a report from September 4th 2013, where researchers are claiming that they may have developed the first reliable method of diagnosing chronic fatigue syndrome by assessing the results of measurements which they obtained from patients by using procedures which were exactly the same as those used in the 1982 project (see my report here), except that the patients on the stationary cycle were attached to breathing apparatus (here) instead of cardiographs. The article is from a website called HealClick, but does not say who the authors of the research were, and the title is “One Test Separates MECFS from Controls with 95% Accuracy“. (end of quote). Note that my results were 100% accurate because the people on the oval were running in exact order from 1st to last, according the measurable data from their laboratory data. This is a quote from their methods together with a photo of their ergometric cycle and attachments . . .
This is another quote from their article . . . “The key measurements for this study are: the Volume of Oxygen consumed (VO2): VO2 max, VO2 peak, VO2VT . . . the amount of work done, measured in Watts: W max, W peak and W VT” (end of quote). When they tested the patients on the first day they didn’t find much difference, but on the second day they found . . . “A decrease in oxygen-consumption function, workload capacity and ventilation was found during the second-day test only in the CFS patients” (end of quote) Here is another relevant quote “Anaerobic/Ventilatory Threshold” . . . A critical factor is the anaerobic threshold, the point at which the body has to supplement normal aerobic (oxygen-burning) metabolism with much less efficient anaerobic metabolism, creating lactic acid (that stuff that if it builds up can make you feel awful). This threshold is measured in CPET by finding the point where carbon dioxide (CO2) starts to be produced faster than Oxygen, it’s called the Ventilatory Threshold (VO2 VT). (end of quote). Compare that again with my report on what happens to breathing during exercise here. This is another quote . . .”Whether this becomes the biomarker test we’ve all been waiting for, the hope is it could help patients in other ways by proving disability or helping to figure out the thresh hold at which their body will go into a pem-crash. Either of those two alone, would be a win.” (end of quote). Note that I have been describing ways of preventing the adverse symptoms which they call “pem-crashes“, based on my own personal experience with limitations, plus the scientifically proven data from my research project since 1982, and earlier, so there is nothing knew about the concept. I don’t wish to bore my readers, but have a look again here. It is a 10 minute Youtube video. They may not be aware of my research, but they do not have the right to make such a claim about being first, although they can continue to do that useful study, but they must acknowledge that I proved the general idea first, otherwise they are committing the crime of plagiarism. I proved that the exercise limitations were directly related to physical working capacity as measured in scientifically verifiable ways. Anyone who uses my ideas or methods in any research since 1983 has either copied me, which is a criminal offense, or has drawn similar conclusion and does not own that idea, and for them to claim that they determined it themselves is only good as verification of mine, and anyone who claims to have obtained the ideas from someone else is committing the criminal offense of aiding and abetting copyright thieves. There are many research studies which are much more closely aligned to my observations and research results which show that CFS patients have breathing, and other abnormalities which relate to limitations to their capacity for exercise that are physical, measurable, and verifiable as methods of diagnosing the ailment. Consequently anyone who refers to my ideas or methods in any research paper, newspaper or magazine article, TV show, or the internet, or public talk, or unofficial or official guidelines or policy, or in any similar manner is committing a crime unless they mention my name as the originator of the idea, or the general set of principles. Some people resent me for defending my rights like that, but they are like criminals who hate the police. I would therefore request ethical and responsible people to recognise how difficult the problem was on the basis that nobody had ever been able to understand it before, and to think about how much time and thought that I put into drawing my conclusions. Thankyou. See my reports on the people who have copied me, such as Simon Wessely, and Peter White of London, and numerous anonymous editors or Wikipedia, and many others. here and here and here etc. Note that the common response that I get is “Oh yes, but that evidence isn’t good enough. The fact remains that it is good enough, and denials are ridiculous. |
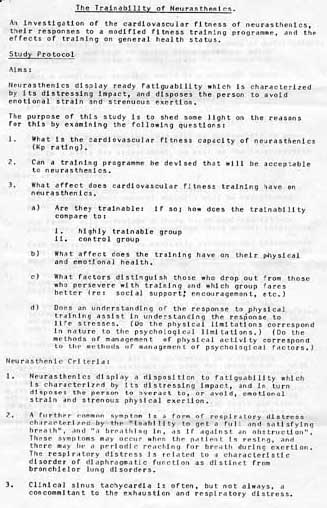
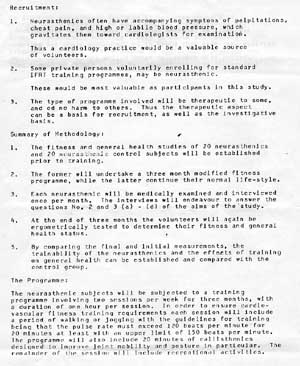

Plagiarism and copyright theft
by Jargon change
The fact that some people have changed the names or invented new labels for my ideas and methods does not alter the fact that they have copied me, or stolen my ideas, or discovered facts or developed ideas after me. They are still my intellectual property and anyone who claims them to be their own idea, or a “New ” discovery, or somebody else’s idea is being either ignorant of the facts or criminal.
When I did my research the standard name fro the ailment was neurocirculatory asthenia, now it is called the chronic fatigue syndrome.
When I advised patients to exercise at their own level and rate, other people invented the label of PACING – run and do other things at your own pace.
When I discovered and scientifically proved that the ailment involved a reduced capacity for exercise, and that the wrong type or level of exercise would cause symptoms, other people called it “effort intolerance“.
When I advised people to exercise and do everything else within their own limits other people gave it the label of the “energy envelope“.
When I advised that patients be educated to learn the difference between their symptoms and those of more serious diseases, and how to adjust their activities I called it “Cognitive Behaviour Therapy“. Modern researchers are still calling it that.
It is obvious to me that they have read my essays, research papers, books, or website and decided to copy those ideas and create the illusion that they invented them as “New” ideas by giving the same discoveries and methods labels that appear to be new or different when in fact they are exactly the same as the ones I invented from 1976 onwards, and scientifically designed and proved in the 1982/3 research project. See here.
How they are getting away with the crime
Other methods which have been used to hide the crime have been to copy my ideas in research projects in other countries, and to do so without consulting me. or telling me, or thanking me, and without acknowledging the fact that I was the source.
Another way they are getting away with their crime is via two Wikipedia editors who were deleting all information about my research so that the only information available to the readers is that of the people who have copied me or come after.
They also described me as a an uneducated and unqualified person, to leave the way open for any person with standard qualification to get the credibility of developing the ideas.
Another process is that which can be summed up by Wikipedia’s policy of consensus where any group of people who out number me can create the illusion that I am at fault, and that I shouldn’t be accusing “respectable” people of such things.
My response
When I wrote my 1982 research paper I knew that I had produced and scientifically proved the value of the idea, and that it was a world first which all future researchers would have to use, otherwise their exercise projects would fail, and I knew that many people would be tempted to steal the idea by pretending it was their own, so I deliberately left out some details which would make the difference between good success, and problematic results. (which is why 51% of patients in the PACE trial are reporting that they were worse afterwards than before.
I didn’t know that my ideas were being stolen with any certainty until I joined Wikipedia in 2007, and then I decided to stop publishing my ideas which had been in development since 2005, I also stopped publishing anything new for a few years, but that was a waste of my time, so I started presenting them as mixed acronyms which would be completely impossible for anyone but me to interpret. See many examples on this page here.
However that presented another problem, namely that when people with CFS etc ask me what to do about their ailments I only tell them what has been published by me, and already stolen, and not latest and best methods.
If anyone wants to know how I solved those problems they will have to guarantee that I get the credit for my original research, and for anything else I tell them.
The copyright thieves have stolen what I have published as if it is an abandoned house after a bush fire, but they can’t steal anything else or even guess without making a hodgepodge of mistakes.
For example, a psychiatrist like Simon Wessely, and laboratory scientists who study with microscopes and x-rays want people to believe that they discovered what happens to people during life, from one decade to the next. The simple fact is that they can’t, and that I many decades ahead of them, in terms of experience alone.
My research is more efficient than most of the studies I read about, and I am willing to co-operate with anyone who wants to gain my knowledge, but I am not going to give it away to grubby thieves.
A modern video of CFS research since mine of 1982/3
The link to the 10 minute You tube video below was provided by Tom Kindlon on Twitter on 20-10-13
The video is about the GP conference: Future NHS services for CFS/ME patients in Northern Ireland dated 23-3-2013.
It includes a discussion on disability by Dr.William Weir, and a talk by Dr.Greg Purdie on The Scottish Good Practice Statement on ME-CFS, and Dr. Charles Shepherd on The Scene in Great Britain who talked about the need to get all existing and new researchers together to solve the problems, and Horace Reid who gave a talk on The Patients Perspective who mentioned that it was “not a good experience” and that as far back as 1996? the Royal College of General Practicioners, and psychiatrists and physicaians warned that CFS was not a psychiatric condition and that nearly all studies showed that between a quarter and a third patients with CFS did not fullfill any criteria for psychiatric disorder. He added that NICE take the same view. He said that CFS patients have capacity and that health care professionals should recognise that the person with the condtion should be in charge of the program. He also said that it was disappointing that so far the NHS has only come up with research providing patiens with coping strategies. That won’t do, he said, “What we want is a cure, and we won’t have a cure until we work out the pathology of the disease is, and that instead of putting all of the money into psychiatric research. a welcome change of direction at the medical research councilin research toward the cardiology and automic function
By viewing this video you can see the discussions amongst various researchers 30 years after I did my research.
Most of what is being discussed is about topics which I have already mentioned in my essays, books and website. There is nothing new about any of it.
The “coping skills” which they refer to were invented by me, because they didn’t exist until I started developing them, and there is the comment that patients now want “more” than coping skills, and that they want research into a “cure“.
They don’t mention that “coping skills” are a lot better than nothing.
They also discuss the funding of research projects, so it would be relevant to say that I organised my the 1982 research project myself and did it for free, as a volunteer, because the funding of my salary wasn’t available, and the institute couldn’t afford to pay me for a project that had not yet been proven.
I therefore proved it for free, and it is the one that the highly funded research scientists, institutes, and doctors use today without paying me a license fee.
They also talk about the modern idea that in many patients it has nothing to do with psychological factors as it was thought to be in the past.
They also talk about three levels of CFS from mild to severe, and comment that modern patients are still having difficulty getting pensions etc. They say that there is no way of diagnosing the problem, but my research clearly indicated that it can be determined by exercise tests, and I also recommended tilt table tests.
In 1975 I was told that there was nothing physically wrong with me, and to go back to work and work hard or be sacked, so I had to resign without superannuation benefits etc.
I scientifically proved that it was physical, which is why all of the changes have happened since.
Most patients have got no idea of how lucky they are now compared to how bad it was before I started. See also here.
Note, that if they want all of the “existing” and “new” researchers to get together, they could send me an invitation, and I would be happy to be there..
The patients perception of fatigue and disability
One of the questions about chronic fatigue is whether or not the patients perception of fatigue is reliable or an exaggeration or normal symptoms.
To answer that question I looked at the scientific measurements of aerobic capacity in their medical files and placed each person in order of fitness.
I then phoned the instructor and asked him to tell me who was running in first place on the training track, and then who was coming second through to last.
He did not have access to the records and did not know the details.
However, the person who he reported as running first had the highest aerobic capacity, and all of them were running in the exact order of the scientific results, and the person who was coming last had the lowest.
They were perceiving their capacity and fatigue with 100% scientific accuracy in a situation where it was impossible to fake.
See also a description of the scientific methods of measuring fitness in ways that cannot be faked here and here.
Terminology and Newspaper Reports
One of my tasks as research co-ordinator was to have some articles published in newspapers to invite
volunteers to join the project. I arranged that by meeting Diane Beer who was a medical journalist for the Adelaide “News” which circulated throughout South Australia.
Fitness helps in therapy
By Diane Beer
SA could have a world first with a fitness research program into a medical complaint which causes abnormal tiredness and depression. The Institute for Fitness Research and
Training today announced a program aimed to relieve the chest pain, fatigue and depression of sufferers while researching the effects of exercise.
Tests
Soviet research assessed the fitness levels of people suffering the complaint, and in Sweden experimental courses were held for sufferers. But neither country assessed the physical effects of exercise comprehensively.
Program co-ordinator, Mr. Max Banfield, said the condition was difficult to diagnose, and many doctors did not recognise the complaint.
The illness has been known by many names over the years and is sometimes called an anxiety neurosis, he said.
Patients suffer heart palpitations although tests show no heart problems.
The News, Thursday, August 5, 1982, page 13.
Study lifts fitness levels
By Diane Beer
The fitness levels of people suffering a rare complaint which causes abnormal tiredness and depression may have been lifted by an SA study.
The pilot study at the SA Institute for Research and Training may be a world first.
People suffering neurasthenia were recruited to the program to research the effects of fitness in reducing chest pains, fatigue and extreme anxiety caused by the complaint.
The study coordinator, Mr. Max Banfield, said one man previously considered too ill to run would take part in The News City-Bay Fun Run after lifting his fitness level through the course.
Mr. Banfield said Soviet and Swedish research into the complaint matched initial findings in SA.
Initial
The fitness course was an extension of initial research.
A general improvement in health was gained in people whose fatigue was attributed to stress.
Mr. Banfield said the condition was difficult to diagnose and many doctors did not recognise the complaint.
He said the illness was often known as an anxiety neurosis because patients suffered heart palpitations although tests showed no heart problems.
Some patients suffered neurasthenia following a severe emotional trauma and continued to experience symptoms years after suffering the initial emotional upset.
The pilot study was very, very encouraging, Mr. Banfield said
He said the majority of people who undertook fitness training at the Centre gained measurable benefits and the study would continue when further funds were available.
The News, Thursday, August 11, 1983, page 13.
During our discussions I needed to identify the nature of the ailment being studied so I described the chest pains, breathlessness, and fatigue, with specific reference to abnormal tiredness, or more particularly problems with physical exertion.
The term neurasthenia had been in common use for about 100 years, but I knew it as Da Costa’s syndrome, and when I was studying the condition I was using research journals which most commonly referred to it as neurocirculatory asthenia.
For the purposes of the newspaper article the term ‘neurasthenia’ was chosen.
I also explained that many of the patients were worried about their symptoms or became depressed because of the limitations to their lifestyle that was imposed by their persistent fatigue, and later mentioned the findings of the interviews with examples of participants who first noticed their fatigue after a viral illness, a prolonged physically exhausting event, or an emotional trauma, so those factors were included in some of the news reports.
I reported the results of each successful three monthly programme so that further articles could be written to invite more participants, and provided the scientific measurements which established that the fatigue was confirmed as a real physical and measurable ailment.
The journalist was required to verify all of those findings with the head of the Institute before publishing the articles.
When I had accomplished the task I had set out to achieve I decided to leave the programme.
A few years later I became aware of comments in the media, particularly radio, about a supposedly brand new ailment called the “Chronic Fatigue Syndrome”, but it was obviously just a new name for the same condition that had been around for hundreds of years with the label changing regularly. (the term CFS had been coined thirty years earlier, in the 1950’s, but didn’t get into general literature).
I later found that there had been more than 3000 research papers published on procedures called “Graded Exercise Training” and “Pacing”, which use exactly the same principles that I developed in the IFRT programme i.e.the participants gradually increase their level of exertion while staying within their own limits etc.
That method has been reported as being the most effective treatment according to surveys of chronic fatigue patients.
It might not appear to be particularly unusual except that most previous programs were dismissing the possibility that patients had physical limitations and were advising them that all they had to do was ignore their symptoms and run as fast as they could to get well. As soon as those people ran past their limits they would experience the distressing symptoms and drop out of the course, so someone needed to design an exercise regime with limits, which is why I was successful.
Some brief notes on criticism of this method
The purpose of doing the research project was to confirm what I already knew in a scientific manner that was proper, constructive and reliable
However, nobody can do anything new without attracting critics.
The first criticism is that the exercise project doesn’t provide a cure, but that does not take into account that there had never been a cure before anyway, and that the project was aimed at getting people to train for 12 weeks or more to determine if there were any benefits from such training. Nobody had been able to achieve that research objective before.
The second is that some patients in similar exercise programs since have reported adverse affects. However, that would not be due to any fault in my original design, but would be due to more recent studies where patients were required to join the course when they were not able to, or where they were required to exercise above their limits.
In my design the patients didn’t have to join if they thought that they couldn’t exercise, and those who did were free to slow down, stop, rest, or drop out at any time. They were not required to do anything that caused them problems.
See more details below.
A comment on research news about exercise and CFS in The Weekend Australian 26-3-2011
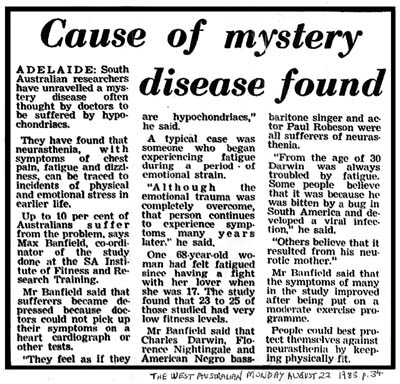
I provided some comprehensive information about the IRFT programme to a freelance journalist in 1983. He sent items to several newspapers including The West Australian Newspaper, which was published on August 22 1983 page 34.
He mentions that physical or emotional traumas and viral infections can sometimes be followed by fatigue which persists long after those events occurred, and that the study found that many of those patients gained a benefit from the fitness programme. See also here
The success was due to the fact that I designed it to include the specifications that no-one had to train if they didn’t want to, and that those who did were requested to determine and keep within their own limits.
An article in the Australian by journalist Tony Kirby presents some information about modern research into the topic of PACING and whether or not it is useful as a treatment. There were some discussions about how to select patients and complaints that the exercise often resulted in problems.
I can give some information form my own experience to clarify some of those confusing issues.
First of all I was a gymnastics instructor who had been keen on sports for ten years prior to developing the problem of fatigue, so it was not due to laziness or the lack of exercise (which is also called ‘deconditioning’)
Secondly when I stayed within my exercise limits (which was slow walking at first, and some slow jogging later) then I was able to continue to improve without problems. However, when i participated in a relay, and squatted down with a medicine ball between my knees and hopped for about ten yards, my heart began to pound violently, and I fell to the ground gasping for breath. It took me about 20 minutes to recover, and i didn’t resume exercises again until a week later. I know from a matter of pure sense that most people who had that experience would leave such a course and never go back.
My fitness levels were measured at the start, and after three months of regular training, and at six months, and were based on scientific graphs of pulse rate over effort, so cannot be faked. The level went from minus 10 to plus 350kpm’s after three months and did not improve despite increasing the frequency and pace of exercise, so I had a physical limitation that was not going to get any better, and was still less than half normal.
The initial reading of minus 10 was because of the severity of my fatigue, and because the graph was drawn as a straight line instead of a curve at the base. Therefore my actual level was estimated at somewhat higher than that, as plus 10.
The plain fact was that it was obvious to me that I had physical limitations and didn’t need to get ‘scientific’ evidence of it. That is just what other people need to verify it.
The physical limitations meant that it was possible for me to exercise at a slow pace, and impossible to exceed my limits, which meant that I didn’t sprint or lift heavy weights.
I did the training purely because I thought it was a good idea, and not because doctors or anyone else suggested it, and my sole purpose was to get back to normal health, but it turned out that it was not possible.
Consequently I didn’t know that, according to some opinions, I was supposed to have a fear of exercise (nobody told me that), and I didn’t have a fear of exercise, and I didn’t have anyone else telling me what I ‘should’ or ‘should not’ be able to do, or force me to exercise past those limits. I just did what was sensible, practical, and possible.
It was obvious to me that I had a type of chronic fatigue which was directly related to a physical impairment which also reduced my capacity for exertion.
Five years later I was asked by the head of the research institute to design a fitness programme to scientifically study the effect of exercise on other people with chronic fatigue. The results from about a dozen people who continued to train, confirmed that other individuals had similar limitations in exercise capacity, and that they could participate in an exercise programme if it specified that they stayed within their own limits.
The fact that such limitations exist is also evident from a thorough search of the history of medical literature.
It surprises me that modern researchers don’t set exercise capacity as a specific criteria for one type of CFS and separate it from the other types, such as anxiety or depression etc.
Also some researchers expect that the exercise programme will cure every patient, but that is simply not possible. Nevertheless some improvement is beneficial.
They also may not be aware of the history of such research which shows that patients develop adverse symptoms as a result strenuous exertion, and that programs which are designed to encourage or force them to increase their level of fitness have failed repeatedly and had to be abandoned.
The people who designed such programs were at fault, because they didn’t understand the problem, and used the wrong exercise principles, and sometimes, rather than admit to it being due to that factor, they blamed the patient by referring to them dropping out and becoming “therapeutic failures”. (a clear case of victim blaming)
I also suspect that some researchers are deliberately organising the wrong types of exercise programs in order to create confusion.
This is a quote from another source which is relevant the process of producing research results that are deliberately rigged from the start . . . ‘the manufacture of scientific doubt’.
Note also that I gave the freelance newspaper reporter an account of many different causes of the ailment including excessive and prolonged exertion, viral infections, emotional factors, and unknown causes etc, and he, or the editors in charge of each newspaper picked which examples to use, and they generally focused on the ’emotional factors’ rather than the others.
One of many newspaper reports about my research can be seen at the top of this essay.
A copy of a newspaper article about a different study can be seen here
http://sacfs.asn.au/news/2011/03/03_28_putting_exercise_through_its_paces.htm
See also one which questions the value of exercise in chronic fatigue here
http://www.mja.com.au/public/issues/181_10_151104/letters_151104-6.html
See another report on these issues in The West Australian Newspaper’s internet page called “the west” at 12:05 p.m. on February 18th 2011 here http://au.news.yahoo.com/thewest/lifestyle/a/-/lifestyle/8868468/chronic-fatigue-treatment-questioned
The following words are quotes from The Australian newspaper about another more recent study
“ME-CFS is generally defined by persistent fatigue unrelated to, but often worsened by exertion, with other possible symptoms, for at least six months. The condition has long been controversial, in part because of disputes over whether its cause is physiological, psychological or both.”
“They then received one of three treatments on top of this.
The first, adaptive pacing therapy, generally preferred by ME-CFS patients groups, encourages patients to fit their activity level to their energy limits, identifying and so avoiding activities that worsen their symptoms.”
“Some patients fear the $8 million PACE trial, published in British medical journal The Lancet earlier this year, will put pressure on sufferers to be more physically active than is good for them, possibly causing relapse.”
“Critics warn that the PACE findings cannot be applied to all patients because they excluded severely affected housebound patients, and children.”
“Lloyd believes any harm comes from patients not sticking to their agreed plan.”
My comment – Useful information about the effects of exercise in chronic fatigue can be found in a book by Sir Thomas Lewis, which was published in 1919.
References:
Lewis, Sir Thomas] (1919). The Soldier’s Heart And The Effort Syndrome 2nd. edition. New York U.S.A.: Paul B. Hoebe
Lewis, T. (1918). “Observations upon prognosis, with special reference to a condition described as the “irritable heart of soldiers””. Lancet i (181-3)
and here Osler, Sir William (1918). “Graduated exercise in prognosis. Letter.”. Lancet (1): 231.
and by reading other references that I provided at the end of the article here
For more information on the history of CFS see here
|
The Banfield Recommendations based on my research between 1975 and 1984 There are various types of fatigue associated with numerous different symptoms which have been given many different labels. However, if there is an abnormal pattern of sleep throughout the day and night, and if there is an abnormal physiological response to exertion, then the chronic fatigue can be easily, reliably, and scientifically diagnosed by ergometric exercise tests, and tilt table tests. See here and here. Typical and misleading comments from other websites are these – ‘the diagnosis of CFS is difficult’, and ‘there is no diagnostic laboratory test for it’ etc. here |
A laboratory method of causing CFS
Every doctor sees hundreds of patients with this condition every year, so they know that it is real and physical, but for reasons of their own they like to give the impression that it is trivial, imaginary, or mental. I have therefore asked some of them this question . . . “Will you come into a laboratory with me, and let me subject you to some experiments which give you this ailment permanently?”. . . . They all say “No!” . . . When i ask them why they say that doing that type of experiment on humans is unethical. However, as you can appreciate, there is nothing particularly unethical about me doing something with the other persons permission. The real reason is that they know that the condition is real, and physical, and in many cases there is no cure, so it will interfere with their social, sporting, and occupational activities for the remainder of their lives. They will also have to deal with the prejudices of other people such as themselves, and they know how bad that will be.
Introduction to scientific exercise testing for CFS
In 1975 I was having extreme problems with my health which included a reduced capacity for exercise, however, I heard about an organisation called the South Australian Institute for Fitness Research and Training, where people could exercise under medical supervision, so I enrolled and began training twice a week. I was always coming last in walking or jogging sessions, and I knew that most people with my ailment would become embarrassed or discouraged, and drop out of the course, but I persisted. I had to stop training about a year later when I injured my knee, but in the meantime, my fitness level had improved, and although it was still considerably below normal, it had made the condition easier to manage.
In the meantime I learned that the name of the condition was Da Costa’s syndrome, which was also known as ‘neurocirculatory asthenia’. Some years later, while reading a medical book I noted a statement that it was not possible to get effective results from research studies on that subject because the patients ‘could not, or would not train‘. That statement was an indication of the general attitude that the patients did not actually have a physical impairment, but were simply suffering from a mental disorder which involved a ‘fear’ of exercise.
I therefore knew that the popular assumptions were wrong and that the symptoms were not due to a ‘fear’ of exercise.
A few years after that I met Clive Thelning, a friend of mine from my education at the South Australian Institute of Technology, and when asking the usual questions ‘what are you doing now?’ I mentioned that I had been studying the ailment and had a few ideas about it. He said that he actually knew Tony Sedgewick who was the head of the South Australian Institute for Research and Training, and recommended that I discuss my ideas with him.
I told him that the director of a research organistation would not be interested in talking to a person like myself who had no formal medical education, but he persuaded me to contact him anyway.
When I rang the head of the Institute he was quite enthusiastic about the ideas and invited me to attend a meeting where we discussed them in some detail. He said that he would talk to his medical research staff about the prospects of adding a training programme for ‘fatigued’ patients. A few weeks later we had another meeting where he explained that they were too busy with other projects, but then he invited me to co-ordinate the study.
When I advised him that I wasn’t healthy enough to do such a task, and that I wasn’t medically qualified anyway, he said that it wouldn’t matter, because his researchers would do all of the medical examinations and that one of his experienced trainers could run the actual exercise programmes to my specifications at their venues, and that all I would need to do would be collect and compile the results. I thought about his suggestion for several weeks and considered that if I didn’t do anything that this ‘solvable’ mystery, it would continue to be unsolved, so i designed the research programme and submitted it. He accepted the concept and, after some standard formalities were dealt with, the project started.
As each programme was successful another followed until about a dozen people had completed at least three months training. Hence I had demonstrated that if the programme was designed appropriately the patients ‘could’ and ‘would’ train, and I had proven that their reluctance was not due to a fear of exercise. I had also scientifically proven that they had a measurable physical impairment to their aerobic capacity which, in some cases, would benefit from exercise.
When the study increased from 20 patients to about fifty, and then eighty, the workload was affecting my health adversely so when I was asked to increase the study to 200 patients to ‘influence’ world opinion, I left the programme.
One of the medical editors of the Adelaide “News”, Diane Beer, had written several articles to recruit patients with persistent fatigue to the course, and a freelance journalist had reported the general findings in several major interstate newspapers, but I also wrote a research paper which included all of the detailed results and submitted it to two medical journals. However it was not accepted for publication, so I put it in my fiing cabinet.
Nevertheless, i knew that the success of such an important study would spread internationally through the research ‘grapevine’, and that attitudes would have to changeh, and within a few years the newspapers were reporting a ‘new‘ ailment called the ‘Chronic fatigue syndrom‘ – a medical condition where the main symptom was persistent problems with abnormal fatigue. I later found reports that the most effective treatment was an exercise programme where the patients trained within their own limits (instead of trying to keep up with healthy individuals).
Unfortunately there seems to be some individuals who resent me for doing that project, and they described it as insignificant and worthless, and tried to deny or hide the fact that it actually happened, and to portray me as some kind of ignorant fringy kook who has all sorts of mental and behavioural problems.
They have never met me and should just accept the facts and stop writing nonsense. if I was afraid of exercise I would not have volunteered for an exercise programme, and if my methods of exercising were not effective then other individuals would not have been able to train, and the same principles that i developed are regarded as the best methods available today – more than twenty five years later.
(In the past it was known that fear increases pulse rate, so it was argued that the fatigued patients were getting an abnormal increase in pulse rate during exercise because of a fear of exercise, rather than the exercise itself. The success of the programme that I designed showed that the patients were not afraid of exercise, and that the abnormal increase in pulse rate during exercise was due to an abnormal physiological response).
|
The Banfield principle of exercising within limits When I began exercising I soon realised that walking and jogging at a very slow pace was possible, whereas running fast led to the problem of abnormal symptoms so I had to choose between doing nothing or exercising slowly. I chose to exercise slowly because it gave me the opportunity of improving, whereas doing nothing was not going to accomplish anything. I didn’t do it to show other people what to do, or to recommend it as I was of the opinion that other people need to make their own decisions based on their own capacity and experience with exercise. However, many years later I saw a poster which captured that method “The hurrieder I go the behinder I get“ That saying also encapsulates how to lead life successfully with CFS. i.e. You have a reduced capacity for life in general, so If you hurry and fuss like healthy people can and do, then you will wear yourself out, so only do what you can, when you can, at a pace that it moderate. To put it another way . . . If your activities are moderate you can sustain them every day, but if you hurry, you will wear yourself out and be useless for months at a time. or . . . There is no known cure, and no quick way of treating relapses of exhaustion, so prevent them. |
|
Many famous people have had the chronic fatigue syndrome includng Charles Darwin, Florence Nightingale, and American singer Paul Robeson. |
For my report on the controversial history of research into this area see here
For an independent overview of the modern CFS research see the video recordings of day one of a National Institute of Health conference here and day two here
See also the improved modern and better informed attitudes to CFS by the medical profession here
The cause according to patient interviews can be seen here
For my YouTube video on a breathing abnormality which is related to this topic see here http://www.youtube.com/watch?v=iGts2nfGtY0
Famous people who have had the Chronic fatigue syndrome
Over the past thirty years I have spoken from time to time with various people about the chronic fatigue syndrome. The usual responses were the same as those of any conversation with courtesy, interest, curiosity or keen interest, depending on the person.
However I would occasionally get an arrogant or even hostile response from people who have never met me, and would not have the slightest idea about what I am actually like, but they act as if they are somehow or other special, or haughty and lofty, and superior in all personal and psychological ways.
They give the impression that they think that they haven’t got the chronic fatigue syndrome because of their intellectual superiority or strength of character, and that if they did get it they would be able to get rid of it by simple will power.
They are deliberately blunt, rude, and dismissive to give the impression that they think that I am just an ignorant, uneducated, mentally inferior, stupid and lazy person who is so far beneath them that they can’t even be bothered talking to me. When I do make comments they say that I am wrong, or don’t know what I am talking about, or that the complicated aspects are beyond my supposedly feeble comprehension.
In response to such remarks I was curious to know if famous, highly respected people ever had this problem, and when I found them i mentioned them in my books or website.
The qualifications of such people, and their level of intelligence, and their strength of character, and respect in life are far higher than anyone who is ever likely to criticise me.
Michael Crawford had the chronic fatigue syndrome
The actor Michael Crawford, became famous for his role in the television series called “Some Mothers Do ‘Ave ‘Em”, and later for his roles in “Phantom of the Opera”. He then had a role in P.T.Barnum where he became very fit at the age of 38 because he had to learn and perform the circus skills such as the ‘flying trapeze’. He then performed in a musical called “Woman in White”, where he played the role of an obese man called Count Fosco, and had to wear a fat suit which made him sweat about a pint of fluid each time. As a result he gradually became more and more fatigued and he said that he then had some type of viral infection like the flu and developed the chronic fatigue syndrome. He said that his doctors were unable to explain the problem and the pills were not helping so he decided to leave the show and move to New Zealand to get some complete rest for about two years. He gradually regained his strength and sense of well-being, and returned to the stage to play in The Wizard of Oz.
Michael Crawford’s experience is further evidence that what I was saying thirty years ago was correct. Namely that the symptoms of chronic fatigue are real. They are not imaginary, or due to laziness, or the fear of exercise, or the lack of exercise, or from a bad breathing habit caused by the lack of exercise, or from a personality disorder. The condition is also not trivial, imaginary, or all in the mind, and it is not just normal tiredness, or an appeal for sympathy, and is not fake or due to malingering,
My main theory about the cause of fatigue is postural pressure on the air in the chest which impedes the upward flow of blood, and hence strains and weakens the blood vessels below the chest so that there is a weakness of blood flow which results in abnormal tiredness and exhaustion. Since then I have made many other suggestions and modifications to that idea. For example in 1871 J.M.Da Costa described how some soldiers collapsed and fell out of line while marching up and down hills and carrying heavy knapsacks for several weeks while being poorly fed and having viral infections. I have suggested that one possible cause is that they became dehydrated from the sweat and fever, and that prolonged reduced blood volume may have contributed to the weakness of their blood vessels and blood flow to produce the chronic fatigue.
The severity of their condition varied, where some recovered after a few months complete rest. However, most of them only experienced a moderate improvement in their health, and still had some problems with tiredness and fatigue twenty years later. A radio interview with Michael Crawford can be found here
The Countess of Mar
On October 11th 2010 the Countess of Mar delivered an address to the British Parliament in the House of Lords in which she reported that she had been diagnosed with ME (myalgic encephalomyelits) resulting from organophosphate poisoning. The speech was reproduced on the ME association website by Tony Britton on October 12th 2010 here.
The opening words to her speech were as follows . . .
“My Lords, the noble Baroness, Lady Gardner of Parkes, has chosen an appropriate moment to table this Question and I am grateful to her. I declare an interest, as I have a diagnosis-finally-of organophosphate poisoning leading to autonomic dysfunction. I am a patron of several charities and groups that represent the interests of patients with myalgic encephalomyelitis, also known as ME or CFS, but which I will call by its common abbreviation, ME. I am also chairman of Forward-ME.” (end of quote).
The following words are from her closing paragraph . . .
“I wish I had the solution to the suffering of people with ME. It seems that, no matter how often Ministers and senior officials confirm their acceptance of the seriousness of this condition, nothing will change until the culture both within and outside the NHS changes”. (end of quote) See here
BBC radio composer John Rutter
In 1975 I was told that there was nothing wrong with me physically, and that I should ignore the symptoms of fatigue etc, and just keep doing everything the same way I always had, and exercise and run faster and there would be no problems.
However, I had to start doing my own research and develop the methods of doing the exact opposite to that advice, by completely changing my lifestyle to get more rest, and to exercise at my own pace to avoid problems. Seven years later, in 1982, I was invited to do a research project where I scientifically proved the necessity of such changes , and the effectiveness of my method of treating it. The results were widely published throughout Australia in essays, and newspaper reports, and some of those essays would have been readily available overseas. They would have been seen and tested by researchers and patients who knew that the old methods were not effective.
I also had to manage my own health problems efficiently, so when I was asked to increase the study from 65 people to 200 I declined, and became involved in other activities and research in my own way, and with my own resources, at my own pace.
Some time later BBC radio composer John Riutter developed the chronic fatigue syndrome which he attributed to a previous chicken pox infection which soon left him incapable of working in the normal manner, but he was fortunate, because my ideas had brought about the official introduction of the name of the chronic fatigue syndrome, although it was still being ridiculed as just “Yuppie flu“. Nevertheless there were also support groups, which I assume started after my research made it practical, and John Rutter joined one of them and learned the importance of changing the way he did things from taking on commissions which require rushing to meet deadlines, to doing similar programs at his own rate.
He was treating his ailment the way I had described correctly several years earlier, and found that he recovered after seven years. Some people, but not all recover in that manner, but only if they follow my recommendations.
Needless to say, that if he hadn’t used those methods he would probably still be very ill today.
I found out about his experience on a Youtube video below which was made known to me through a comment by James David Chapman on Twitter on 15-10-12, who learned about it from a chronic fatigue patient who gave himself the ID of Constant F***ing Sh*t.
Other famous people from modern times who have had the chronic fatigue syndrome
Singer Greg Page of the famous Australian singing group called the Wiggles developed the chronic fatigue syndrome but it has been reported as “Orthostatic Intolerance“. See my report here.
Similarly, one of Australia’s best known television journalists, Leigh Hatcher, has written a book about his own experience with the chronic fatigue syndrome called “I’m Not Crazy, I’m just a little unwell“. This is a quote from his website . . .
“in January 1998, Leigh Hatcher lay down for a ten-minute afternoon nap—and woke two hours later feeling as if he’d been run over by a truck. Without warning, he’d plunged into a health crisis that was as devastating as it was mysterious . . . and . . . He speaks frankly about the hurt and betrayal he felt when people questioned whether the illness was ‘all in his mind’. See here.
Other famous people from history to have CFS e.g. Charles Darwin
Charles Darwin, Florence Nightingale, and Paul Robeson. had the same symptoms before the label of chronic fatigue syndrome was introduced.
Some interesting facts:
Charles Darwin was extremely seasick when he sailed on a ship called the Beagle for the first time, as it rocked about in heavy seas during a gale. After returning to port he had chest pain and palpitations which were relieved when the storms subsided. When he set sail again he would often become exhausted by seasickness during storms, and would gain relief by laying in a hammock.
He also may have become ill after being bitten by the reduvid bug that causes Chagas disease, which is a common cause of illness in South America which he visited. That disease has an acute phase, and then goes into remission for many years before the chronic phase occurs. However, it may have been due to being poisoned by tribal chiefs who didn’t like his attitude towards religion.
When he returned to England he continued to suffer from fatigue for the rest of his life. His father was a prominent London doctor who thought that his sons chronic illness was due to the long periods of exhaustion during his ship voyages, and his wife thought that his problems may have been due to anxiety, but Charles said that he was not anxious, and that his problems were not due to the exhaustion from seasickness on his voyages.
I have written the Posture theory to explain the cause of such symptoms, and I noticed that the photos of him depict his very stooped shoulders, and he is often ridiculed by his critics with drawings depicting him as drawings depicting him as a stooped ape. I also noticed that he had a carpenter build a writing platform across the arms of his chair, and a photo of one of his rooms shows a tall music stand, with the platform for the music sheets at a height which would be used for standing up to read, rather than sitting. (I noticed such things after developing the method of standing to read and type to relieve some of my own symptoms. See here. Note also that despite his father being a top London doctor he was unable to prevent, treat, or cure the ailment).
Florence Nightingale is regarded as the founder of modern nursing. She became ill with “Crimean fever” (brucellosis) during the Crimean War. When she returned to England she kept working while exhausted, despite the fact that her doctors advised her to rest or risk chronic invalidity. For much of her life after that she was bedridden, and died at the age of 91. Despite being one of the most useful contributiors to society, the fact that she was bedridden had many people pejoratively calling her lazy and manipulative. Of course that is a ridiculous and offensive way of saying that she was continuing in a situation of adversity.
Paul Robeson was a famous American negro singer who developed the chronic fatigue syndrome
Sportsmen
Alastaire Lynch was a prominent Australian League Footballer and captain of the Brisbane Lions. He had many years of problems with chronic fatigue syndrome but was later able to return and complete his football career,
Raelene Boyle
Former Austalian Olympic athlete Raelene Boyle suffered faintness and fatigue and would sometimes sleep for up to 20 hours per day. For 12 years her symptoms were misdiagnosed as stress induced panic attacks but eventually she was found to have atrial fibrillation and she was given surgery to implant a pacemaker. Since then she hasn’t had any symptoms and has been able to return to the normal activities of a 61 year old woman. See here and here.
Three different approaches to discussing the chronic fatigue syndrome and the “all in the mind” arguments
Most people accept the “all in the mind” arguments for diseases until such times as one of those ailments affects themselves, in which case there are, in general terms, three “normal” and “common” and different types of response.
The first is the tendency to be defensive and argue that they are not mentally ill but have an undetectable physical problem.
The second is the consideration of doctors being respectable people who have completed at least six years of training at university, and have an occupation where they try to relieve the pain and suffering of anyone who has the misfortune of becoming ill. Therefore, the response of intelligent people is to study the ailment objectively and present scientific evidence of a real physical basis for their problems in a manner that is diplomatic and respectful.
The third response is usually not evident until all objective and diplomatic approaches have failed, in which case the person may become critical, angry, or even hostile toward the victim blaming arguments.
There are also other common responses where patients become anxious or worry about their situation, or where they lose all hope of anyone ever understanding or accepting their illness and become depressed.
There are also a number of widely known cliches or stereotypes which are a consequence, and which all such patients will have to deal with sooner or later, and the first is where the doctor says “Are you questioning my authority“, and the second is “So, in your opinion, it is not you that is mad, it is the rest of the world“.
Two types of Chronic fatigue
detectable and undetectable
There are two types of chronic fatigue. Firstly the type where the cause has been found, and the second where it hasn’t.
It is most likely that the majority have a physical or biological explanation, but it is generally argued that those which are detectable are therefore physical, and those which are not ‘yet’ detectable are mental.
The idea that undetectable causes must be mental is ridiculous.
Of course it is possible, but in many cases, just plain wrong, and it is just a matter of time before the real cause is found.
One of the typical arguments I have noticed is very devious and goes like this . . .
“Oh your type has no detectable basis therefore it is a mental disorder.” . . . and . . .
“Oh the other persons chronic fatigue is caused by brucellosis therefore it is not the ‘chronic fatigue syndrome’ which is a ‘diagnosis of exclusion'” (which is only diagnosed after everything else has been excluded). and . . .
“Oh the other persons chronic fatigue is caused by ‘orthostatic intolerance’ therefore it is not the ‘chronic fatigue syndrome'”. . . and . . .
“Oh the other persons chronic fatigue is caused by ‘postural orthostatic tachycardia syndrome’ therefore it is not the ‘chronic fatigue syndrome'” . . . and . . .
“Oh the other persons chronic fatigue is caused by ‘neurally mediated hypotension’ therefore it is not the ‘chronic fatigue syndrome'” . . . and
“Oh the other persons chronic fatigue is caused by a newly discovered real cause, therefore it is not the ‘chronic fatigue syndrome’.
In other words millions of people suffer from chronic fatigue, but the only ones who are given the diagnosis of “chronic fatigue syndrome” have been, and are now, and always be in the future, the ones who have a type of chronic fatigue which isn’t yet proven to be real, so they will continue to be ‘wrongly’ diagnosed as having a psychological, rather than a physical cause.
The problem of misdiagnosis or ‘maldiagnosis’
The problem is that as long as the real physical basis remains undetectable the patients will continue to be treated as if they are just ‘lazy’, or ‘unfit due to a lack of exercise’, or just haven’t had enough sleep, or are just whingers who complain about normal tiredness, or are just fatigued because of constant worry etc. In that regard the diagnosis of non-physical cause actually creates prejudice, and therefore adds an unnecessary problem to the patient with fatigue. Attributing the problem to non-physical factors is therefore a ‘maldiagnosis’ (a harmful diagnosis – one that does more harm than good).
Chronic fatigue – a common condition
Another observation is that 2-4% of the population, or 200 million people have the chronic fatigue syndrome, but there are more than 100 different labels for it, so if 100 different people met, they would each think that they had a different ‘rare’ problem, and never know that it was one of the most common problems affecting humans.
Patients with ‘chronic fatigue’ of any type would have more influence if they were united, rather than split into 100 different groups.
|
The Posture Theory and Chronic Fatigue The first indication that I had that posture had anything to do with my own health problems was when I was working as a public service clerk. I was transferred to the cash controllers office where part of my duties was to sit at a desk and count the daily take of coins into piles of twenty of their particular denomination. I noticed that after a couple of hours of starting work at 9 a.m. that I would get a vague ache in the left side of my back at the level of my left kidney, and if I continued with that work for another hour I would also start getting the ache in the region of my right kidney. A few months later I had some tests and was found to have a stone in my left kidney. About a year later, when I was engaged in my usual pastime of gymnastics, I performed a handspring heels over head leap and when my feet landed on the floor with my back arched I felt a ripping sensation in my upper abdomen. I waited a few moments to see if blood would come pouring from my belly, up through my throat , and out of my mouth, but nothing happened so I resumed my activities as an instructor without any further problems. However in the next month or so, I started to notice that I would get a nagging ache in my belly about an hour after commencing my days work as a clerk. I also noted that these aches were associated with leaning toward the desk to read or write, and that the longer I did that work for the worse the pain got. Hence the pain was worse on the busiest days of the week. Within a year or two the abdominal pain was becoming more of a problem and I was beginning to feel faint, or dizzy or breathless as well, each time I leaned toward a desk. I was also getting fatigue, and one night in the gym I performed an exercise called a round off back somersault and when I landed on my feet I felt dizzy and it appeared as if a thousand stars were shooting in all directions before my eyes, so I stood still and stayed bent over. I then waited for a few moments expecting to lose consciousness and collapse, but I recovered without ill effect and continued with my activities, although in a more subdued manner. The problems were therefore beginning to have a serious effect on my occupation and my lifestyle. Unfortunately the problems were a mystery to my doctor, and the medication that he was prescribing was not helping, as my health continued to deteriorate regardless. At about that time I read that an organisation called The South Australian Institute For Fitness Research and Training was conducting fitness training programmes under medical supervision for various ailments. I therefore thought that I could attend such a course as treatment and that the researchers might be able to enlighten me about the nature of my ailments. At the initial medical assessment I was required to ride an ergometric cycle while attached to electrodes which recorded pulse rate over wheel pressure and could measure aerobic capacity with scientific reliability. The result was a fitness level of zero, compared to a friend of mine who measured 900, and an Olympic athletes measurement of 1200. Another person I met was a forty year old overweight asthmatic with a measurement of 600. At the same session my body fat was measured with calipers, and I was told that I was all skin and muscle, with virtually no body fat, and that I had the muscle/fat ratio of an athlete, probably due to ten years of sport and gymnastics. I trained at the Research Institute for three months and achieved a level of 350 kpms, and increased the programme to four times a week and three months later was still at 350 kpm’s so I concluded that I had some sort of physical impairment which was limiting my fitness capacity regardless of the amount of exercise I did. I trained more often again for another 3 months and then injured my knee cartilage while playing social volleyball with the other programme participants. My leg remained injured due to diagnosis and post operative problems for 3 years. During all of that time I was inquiring about my health and studying it and writing about my conclusions, and submitting my essays to the Australasian Nurses Journal. After several articles had been published I met and befriended the editor, Edna Davis, who continued to publish my articles about once every three months. Five years later I was able to conclude that most of my ailments were aggravated by leaning forward, including the fatigue, and in 1980 I wrote a three page essay called The Matter Of Framework, which I have since called The Posture Theory. Some time later I became aware that Sir Mark Oliphant was living in a nursing home in North Adelaide and I knew that he was regarded as one of Australia’s most respected scientists for his involvement in the Manhattan Project which developed the atom bomb, so I phoned him and arranged a meeting with the objective of asking him his opinion about the theory. At our first meeting he said that he thought the idea was interesting, but that he was not qualified to comment on medical matters with any authority. However he told me that he would discuss it with some of his colleagues who were among the country’s top medical researchers and let me know their opinion. When I met him again two weeks later he advised me that his medical colleagues also regarded the theory as interesting but that it was not possible to say anything other than that because that whole area of medicine (the range of undetectable an unmeasurable ailments) was a Pandora’s box of mysteries. One day, while walking along a city street I met a friend of mine, Clive Thelning, who was blind, and who I had befriended some years earlier when I was studying group psychology at The South Australian Institute of Technology, and I asked him what he was doing. He had completed the Certificate Course, and went on to do a Psychology Degree, and was working as a psychologist. I told him about my essay and he said that he knew Tony Sedgewick who was the head of the research institute where I trained, so he suggested that I approach him with the view to arranging some research on the subject. At a subsequent meeting with Tony Sedgwick I outlined a potentially useful training and research programme for reliably and scientifically assessing the aerobic capacity of people with persistent fatigue, and asked him to discuss it with his research staff to see if they were interested. At a further meeting he advised me that his staff were fully committed to other projects and invited me to run the programme. I told him that my health problems would impede my capacity to do such a project properly, and added that I thought I was not able to do scientific studies unless I had medical qualifications, and that I didn’t know how it would be funded. He then advised me that he had some medically qualified contacts and that I could approach them with the view to forming a committee to satisfy all the requirements of administering such a course, and he gave me the name of a politician who I could approach for funding. A committee was formed and a very small government research grant was obtained so the programme was established. I then approached a journalist named Diane Beer who wrote several articles for the Adelaide newspaper called the “News” inviting people with persistent fatigue to attend the course. After three years 80 people had been assessed as having aerobic capacities of 100 to 1200 kpms with variable responses to training from those who did not participate, to those who trained but did not gain much in fitness, to one who trained for nine months and participated in a small marathon (about 6 miles). My own health problems stopped me from continuing the recording and reporting of the statistics in the programme, but there was also conflicting data which I couldn’t account for. i.e. I expected all fatigued participants to have low aerobic capacity, but some had normal or high levels, and I didn’t understand how that could be so at the time of making my initial report. However, about 5 years later I drew the conclusion that those fatigued people who had low aerobic capacity possibly had a fitness disorder (a disorder of exercise metabolism), and those with a high aerobic capacity must have had a sleep disorder. (In the English language the word fatigue has two meanings: more commonly it means physical exhaustion, but that same word is also used to describe tiredness, therefore, if you recruit people with fatigue into a training programme, then you are likely to get two totally different types of volunteer, those who become readily exhausted by exertion, and those who are always drowsy – you would also find some overlap and confusion of both symptoms in the same individual). Another five years went by when I was diagnosed with cancer and given two months to live with no hope of a cure. The cancer had spread to most of my lymph glands, and was in my blood and bone marrow. I didn’t think that I would be able to study and cure cancer in two months, so I decided to occupy my remaining time by writing about posture and health, and if sitting at a desk aggravated my health problems it wouldn’t matter because I would soon be dead anyway. The task did aggravate my health problems and caused some damage as I wrote one sentence, or one paragraph, or one essay at a time. After about 6 years I discovered that standing and typing in front of a computer screen positioned at eye height caused much less problems than sitting and leaning forward to write at a desk. The book continued to increase in size at about 150 pages per year and 8 years later in the year 2000 when my cancer was cured by a stem cell transplant, I completed it as the 1000 page 11th edition. Over the years several editors have commented critically on my writing style as being an unusual collection of sentences, paragraphs, and illustrations, but I have noticed the advantage of spending a lot of time thinking, and a small amount of time writing. The research project results were submitted to several medical journals in 1983 but were not accepted, with one editor advising me apologetically, that it would need to be re-submitted in the appropriate medical format before being publishable. I have decided to present the results in rough form on this web page 24 years later in April 2007. M.B. |
The history of chronic fatigue syndrome
In the 1980’s I heard news reports of a supposedly brand new disease of modern civilisation called the Chronic fatigue syndrome, but it was only a few years after 1982-3 when I had scientifically proven in Adelaide that chronic fatigue was a physical and not a mental illness . The only thing that changed was the label from neurocirculatory asthenia to CFS. Furthermore, new diseases generally don’t just materialise from nowhere, and in fact the history of CFS can be traced back throughout history at least as far as 1750 when there was a book about it called “Febricula” which means “little fevers“. Similar outbreaks have occurred in more recent times. One example occurred in the nurses and staff of the Royal Free Hospital in London where it became known as the Royal Free Disease. Some people argued that it was due to a virus, but the most widely accepted opinion was that it was an example of mass hysteria. However, other outbreaks have been reported in many other places such as New Zealand where it was called Tapanui flu, and in Iceland where it was called Icelandic disease.
The problem has also been associated by Da Costa to infectious illnesses during the American Civil War, and by many others in World War 1, but other factors and many other theories relate the ailment to excessive exertion, poor food and water supply during long marches, injury and shockwaves etc, but the dominant view was that it was due to psychological factors related to anxieties and fears such as the fear of battle or exercise etc. Nevertheless I scientifically proved that it was a physical illness in 1982-3. See here, and one of my reports here. You can also read about the ailment and it’s history in at least 2 sections of my book here.
See also the Disease of 1000 names website which now lists more than 100 different CFS labels from history here.
Some quotes from history can be seen below . . .
References relating to the Chronic Fatigue Syndrome
A very common illness which has been well known for two centuries
The modern jargon for hypochondria is “Somatoform disorder” which is used to describe ailments which are “supposedly” imaginary or “all in the mind” and there have been many inappropriate and erroneous attempts to apply it to the chronic fatigue syndrome. Those attempts often succeed because most patients don’t understand the jargon, and can’t defend themselves from such entirely fallacious arguments
Many doctors and medical experts continue their attempt to create the public impression in their journals, and in newspapers, and on their websites that CHRONIC FATIGUE is a very new and quite rare condition. They imply that there has never been any scientific evidence of it having a real or measurable physical basis, and that therefore there is a great deal of doubt about whether it actually exists or not. It is still widely reported that the condition is just normal tiredness which some patients complain excessively about, or that it is “all in their mind“. Many doctors also persist with their disproven suggestions that the condition can be cured simply by thinking positively and doing some sort of exercise or another. I do not wish to comment on why they try to create this false, and insidious, and pernicious impression but I will present some quotes from medical publications of the past to discredit that deceit.
The chronic fatigue syndrome is one of the most common diseases of modern life but it is not a new condition. In the past it has been given many different names which include DaCosta’s syndrome, neurasthenia, neurocirculatory asthenia, vasoregulatory asthenia, and the effort syndrome etc. Here is some information from the past which has been extracted from the 11th edition of The Posture Theory.
“The patient’s voice falters. ‘Doctor, I’m so tired. What’s wrong, what shall I do’.
Every hour, every day, in almost every doctor’s consulting room, at least half the visitors voice this complaint.
Of all ages, of either sex, rich or poor, they make up the vast throng of fatigued human beings who get little comfort from the pills, shots and examinations they solicit from baffled physicians”
From: Our Human Body, It’s Wonder and It’s Care (1962) p. 410
“Neurasthenia”: This diagnosis “had wide popularity in the nineteenth century and is now obsolete. It referred to a state in which the major symptoms were chronic fatiguability, lack of endurance, backache, and headache”.
From: Harrison’s Principles of Internal Medicine 6th Edition (1970) p.1863
“Neurasthenia is a term which, in the past, was used more commonly as a diagnosis than almost any other”. Now it is used only for cases of “execessive persistent fatigue” where there is no evidence of pathological cause.
Reference: The British Encyclopaedia of Medical Practice (1950) Vol.10, p.32.
Neurasthenia . . . The classic neurasthenia patient is thin and underweight and “wanders from one physician to another seeking relief from various complaints and may undergo unnecessary surgery or extensive medical treatment on insufficient or vague indications …. Changes in lifestyle … and ‘rest cures’ along the lines of old-time spa therapy are of value in some cases.”
Reference: Current Diagnosis And Treatment (1973) p.574.
“Neurasthenia is a state of chronic mental and physical weariness for which there is no obvious cause.” They feel tired “as soon as they attempt to undertake the ordinary tasks of life” and when they do manage to work it is below their previous standards.
They awake “tired and unrefreshed” and are at their worst in the morning except when “they have to work hard, in which case the amount of tiredness is out of proportion to the amount of work performed.”
There are many accompanying symptoms including headaches, palpitations, and indigestion, and . . . “Reading makes their eyes ache or produces the sensation of spots in front of their eyes.”
Reference: The Universal Home Doctor (no date) p.531.
In the 19th and early 20th centuries people who suffered from pain and fatigue or paralysis were diagnosed as having ‘nervous spine’, ‘neurasthenia’ or ‘fits’.
Edward Shorter called such people “somatizers” and described them as suffering from “pain and fatigue that have no physical cause”, and suggested that they were playing sick as a means of consciously or sub-consciously seeking solace, attention, or social excuses.
“Such somatizers have produced a fascinating succession of phantom diseases” and the “Archetypal Victorian ladies” collapsed on their beds, or had fits, convulsions, or paralysis, but, “By 1900 such operatic displays softened into a symptomatological chamber music”, of less dramatic symptoms of neuralgia, headache, and fatigue.
Such patients were “frustrating to no-nonsense physicians such as the early twentieth century Kentucky doctor” who believed that “a good spanking”, or sometimes even a “good cussing” was the best treatment for such “evident hypochondriacs”.
Nowadays the condition is called “myalgic encephalomyelitis or ME (also called ‘yuppie flu’ or chronic fatigue syndrome)”.
Reference: The Cambridge Illustrated History of Medicine (1996) p.111-112.
“The neurologist calls the disease, in technical phrase, neurasthenia; the gynaecologist is too likely to look no farther than the womb and ovaries; and the general practitioner is apt to imagine spinal disease, dyspepsia, “liver complaint” or “malaria” to be at the bottom of all the trouble. Each treats the patient from his partial stand-point, and is disappointed that recovery does not result.”
From: The Ladies Guide (1904) p.588-589
The psychiatrist divides these individuals into groups of “anxiety states, obsessional neuroses and conversion hysterias.”
These conditions include the effort syndrome (chronic fatigue) and may occur “in the convalescent period after such acute illnesses as influenza, pneumonia or even tonsillitis, particularly in young adults.”
A hasty convalescence predisposes to this condition so “special care” should be taken in determining the appropriate time for returning to work.
The condition causes “distress, disability and economic incapacity” and has an intractable nature.
“Drugs are of little or no value.”
Reference: Textbook Of Medical Treatment, 4th edition, (1946) p.604-606.
The most common symptom in neurasthenia is ready fatigueability, but there can also be headaches, dizziness, ringing in the ears, palpitations, chest discomfort, cold feet and hands, digestive disturbances, constipation, sleeplessness, and “pains in the neck, between the shoulders, or in the back and the limbs, with tender spots along the spine”. “In fact the symptoms are so many and so varied that it is common for a neurasthenic to imagine that he has any or every disease that he happens to read about.”
Reference: Modern Medical Counsellor Revised Edition (1957) p. 554
The Chronic Fatigue Syndrome has previously been called many things, including the Effort Syndrome because it often involves “effort intolerance” and “is characterised by a group of symptoms which unduly limit the subject’s capacity for effort”. Breathlessness 93%, palpitations 89%, fatigue 88%, left inframammary pain 78%, dizziness 78% and or faintness 35%.
Reference: Diseases of the Heart & Circulation 2nd Edition (1956) p.937-944
“The pulse is always greatly and rapidly influenced by position . . . Dizziness was often complained of”. It was increased by stooping (case 44); by exercise (case 57) or by laying on the left side in some cases or on the right side or the back in others. For treatment . . . “Their equipments be such as will not unnecessarily constrict and thus retard or prevent recovery”.
Reference: Da Costa J.M. (January 1871), On Irritable Heart, The American Journal of the Medical Sciences p.18-52
Erben’s phenomenon . . . temporary slowness of the pulse on stooping or sitting down; said to characterize certain cases of neurasthenia.”
Reference: Dorland’s Illustrated Medical Dictionary 25th edition (1974) p.1179.
Neurocirculatory asthenia, Da Costa’s Syndrome is less adequately called “the soldiers heart”, the “effort syndrome” and “anxiety neurosis”, and involves instability and abnormal irritability of the nervous and circulatory system of unknown cause. It tends to be precipitated by physical exhaustion, nervous strains and infections.
Symptoms occur as a syndrome of breathlessness with sighing respiration, palpitation, exhaustion, precordial pain, (or ache), dizziness, nervousness, tremor, sweating, headache and faintness aggravated by effort or excitement. In some cases the condition is more or less constant with little or no provocation. “That such a state of ill-health exists there can be no doubt”. It is not just fatigue, or infection or nervous strain or psychoneurosis, but may attend or follow such conditions “or even frequently stand alone”.
The effort syndrome is sometimes considered unworthy of discussion because “so far as we know, it is not an organic disease, and since it may occur in perfectly normal persons,” but it is important because “it is often a partially or completely incapacitating condition”, and treatment is important but often neglected, and it is essential to distinguish it from organic heart disease. . .
It is a real and not an imaginary incapacity, even though at first glance it may have appeared imaginary during World War I (1914-1918) when it was sometimes labeled “malingering”, and even though in civilian practice it has frequently been diagnosed as “mere nervousness”.
The cause remains obscure, where there are no pathologic changes and the heart is usually structurally normal, and there are no lesions of the nerves or glands, although “Abnormalities of central nerve cells induced by fatigue in experimental animals have been noted and may be possible factors”. . .
Blood pressure may be a little elevated and variable, strength and endurance tests and vital capacity are low, in some cases extremely low. There is an easily induced oxygen debt on exercise with an excess accumulation of lactic acid.
Reference: Paul Wood, Heart Disease 4th edition (1951) p. 579-585
DaCosta’s syndrome . . . “Lewis commented ‘it is because these symptoms and signs are largely, in some cases wholly, the exaggerated physiological responses to exercise . . . that I term the whole the ‘effort syndrome’ . . . ‘a proportion of the patients whom I include in the group effort syndrome sooner or later acquires the diagnosis of neurasthenia.'”
In some cases “the chest is long and narrow or flattened and associated with a kyphotic curve” or the person is slight in build or has chest wall deformities. The pulse shows an exaggerated reaction to posture. The condition can effect soldiers particularly those who came from sedentary occupations and who had signs of the condition in civil life many years before joining the army. It affects sedentary town dwellers and is commoner in women”.
From: Wooley C.F. (May 1976) Where are the Diseases of Yesteryear, Circulation p. 749-751
DaCosta’s syndrome . . . After exercise the pulse rate deceleration time is abnormal.
Reference: Paul Wood, Diseases of the Heart & Circulation, 2nd edition, Eyre and Spottiswoode (1956) p. 940-942
During exercise the breathing rate increases for all people including those with neurocirculatory asthenia, but in those with neurocirculatory asthenia the “breathing becomes disproportionately shallow.” “During exhausting work, such as running, patients developed significantly high blood lactate concentration” indicating “that aerobic metabolism was defective in these patients.”
Since World War I it has been known that high concentrations of C02 can trigger a so-called ‘anxiety attack’ in patients with neurasthenia.
These patients were generally thin and “were poor athletes” and were especially poor swimmers”. . . and their symptoms “are not mentally determined or removable by analysis.”
Reference: Neurocirculatory Asthenia: 1972 Concept, Journal of Military Medicine (April 1972) p. 142-144
The concept of ME (the Chronic Fatigue Syndrome) has deeply divided the medical profession and provoked bitter arguments between those who believe it is “entirely imaginary” and those who think “it has an organic basis”.
Some doctors belittle the condition and regard the patients as malingerers and manipulators.
The condition mainly affects women, but some men also suffer from it, including “both male and female members of the medical profession”, and it features severe fatigue which can “be made worse by exercise, a single act of which may cause fatigue for weeks.”
Reference: Symptoms (1996) p. 300-304
Researchers at the Harvard Fatigue Laboratory in America have ” learned that physical fatigue is caused by a complex chain of chemical reactions” where prolonged muscular effort causes lactic acid, carbon dioxide and other by-products to seep into the bloodstream . . . “So acute is the chemical change that injections of the blood of a fatigued animal into a rested animal will produce fatigue.”
Reference: Our Human Body Its Wonders and Its Care (1962) p.413.
It may be useful to inject the blood of people with chronic fatigue into healthy experimental subjects to determine if they too become fatigued. M.B.
Treatment: “The plan of life of the patient is to be worked out with care. Usually normal but quiet work and play are to be advised, with avoidance of late hours, coffee, tea, over-indulgence in alcohol and tobacco, strenuous vacations, excitement in general, too many hours at work, and new or burdensome tasks or duties. Often the patient himself is aware of this necessity, but he has perhaps disliked to humor his symptoms or to fall behind his fellows in strenuous living in the business, professional, and social world. With clear medical advice, however, he realizes the wisdom of doing so, and gradually he adjusts himself to suit his symptoms, and is surprised at recapturing a feeling of well being.”
Reference: White P.D. (1951) Heart Disease 4th edition, Mcmillan & Co., New York, Ch. 22 (neurocirculatory asthenia) p.587.
The origin of ideas about posture and fatigue
When I first became interested in the study of medicine one of the primary symptoms that I was considering was a form of fatigue. Four years later I was able to recognise that it came on more readily and persisted longer than ordinary fatigue. I likened this to the way one end of a seesaw rose too fast and fell too slowly if the people on each end were of unequal weight. I therefore referred to the fatigue as a disorder of equilibrium, and began writing an essay to summarise that conclusion.
At that time I was also writing an essay on a postural cause of backache, chest pains, breathlessness, stomach pain, and kidney pain. As the fatigue occurred together with this set of symptoms I suspected that there may have been a postural cause for the fatigue as well, but did not have the evidence to establish that fact. I therefore started a third essay in which I brought all of this information together in an attempt to integrate it.
While looking for clues I came upon a word in a Medical Dictionary called Valsalva’s maneuver which referred to an experimental method for stimulating the nervous system. It then occurred to me that overstimulating the nervous system might damage it and cause it to malfunction, resulting in chronic fatigue, so I sought a more detailed explanation of the maneuver at the Barr Smith medical library. I then determined that Valsalva’s maneuver involves holding the mouth and nose shut and breathing out forcefully to increase the pressure in the lungs. This impairs blood flow through the chest and stimulates the nervous system to increase the blood pressure in the arms and legs, which in turn forces the blood through the pressurised chest.
I was aware that the fatigue symptom was common in sedentary workers and rare in manual labourers so I assumed that repeatedly leaning toward a desk hundreds of times a day for many years might be repeatedly pressurising the chest and eventually causing the nervous system to malfunction.
I then discarded the three other essays and started writing one new essay describing how all of the symptoms had a common postural cause. When I was considering several titles I realised that I was writing a framework of ideas to link a framework of symptoms, and I noted that these were related to the framework of the human body, so I eventually decided that one of the best of the title options was The Matter Of Framework, so that is what it was called, and that essay was the original Posture Theory.
I later attended a meeting of a group of people who suffered from chronic fatigue, and they were basing their discussion on the possibility that the condition was caused by a virus.
Since then I have concluded that there are different causes, types, and degrees of severity of the condition. Most, if not all of these conditions involve excessive tiredness, which is a disorder of sleep metabolism, and one type involves abnormal responses to physical exertion, which is a disorder of exercise or energy metabolism. M.B.
Any written permission which has been granted to publish information from this webpage relates to the information above this line. The information below this line is new to this page and may be referred to or linked to, but not published. Acknowledgement of the source is required. M.B.
The Posture Theory:
in progress from 8-3-02
The nature, measurement, and management of The Effort Syndrome
|
The confusing aspects
The possibility that many different problems have been lumped together under the same general fatigue category, which has previously been labeled by hundreds of different titles, has long been recognised, and there have been many attempts to distinguish the sub-groups. This category has included several main groups which include those relating to the function of the circulatory system, the post-viral category, and the psychological possibilities. Hence the same broad group of syndromes has been labeled as neurocirculatory asthenia, myalgic encephalomyelitis, or anxiety state, and there has been a general tendency to lump all people with fatigue in the same way (to fit square pegs into round holes). Hence they have all been deemed by some to have circulatory problems, or by others to all have a post-viral condition, and of course there have been suggestions that they are all anxiety states, or depressives, or are complaining excessively about normal fatigue It is worth noting that all people experience fatigue after strenuous or prolonged exertion, but they usually recover in a few minutes or hours, or by the next day. It is also common to have fatigue during an infectious illness but this usually only persists in the course of that illness, and or in the convalescent period, but in some cases it persists chronically for months or years afterwards. Others notice that when they are anxious they get fatigued, and when the are depressed they may be too apathetic or too tired to get out of the bed in the morning. However, regardless of the number of different conditions which are involved, there is a group of people who have chronic persistent problems with fatigue, and who also experience a set of symptoms in relation to exertion, yet they are not anxious, nor depressed, and some have been former athletes or sportsmen, so the idea that their symptoms are due to a fear of exercise is unlikely. When examining the aerobic capacity of any 100 people with chronic fatigue there are usually a small percentage who have very high aerobic capacity, and this has been customarily regarded as proof that the fatigue does not have a physical basis, otherwise, it has been said, they would all have low aerobic capacity. However, if all the individuals with low aerobic capacity were considered separately as having a specific problem, for which the term “The effort syndrome”is apt, they could probably be identified, not as being contradictory, but as having some consistencies, and some of the confusing aspects of these problems would be solved. Those aspects which are particularly relevant to an effort syndrome are included in the accompanying list. |
The distinguishing features 1. low aerobic capacity 2. defective aerobic metabolism 3. poor breath holding ability 4. reduced capacity for exertion 5. disproportional shallow breathing during exertion 6. readily induced oxygen debt in response to exertion 7. high blood lactate production during exertion 8. sensitivity to high concentrations of CO2 9. ready fatigability 10. fatigue accruing out of proportion to particular types and levels of exertion or strain 11. poor stamina for high levels of exercise 12 inability to sprint for short distances with, in some cases, a concurrent average stamina for low levels of exercise 13. reduced capacity for anaerobic exercise 14. exaggerated response of pulse rate in proportion to effort 15. Slow deceleration of pulse rate after exertion 16. abnormalities to pulse rate in relation to stooping or squatting, or to changes in posture such as standing suddenly 17. abnormalities in the circulation of blood in response to sudden loud noise 18 abnormailities in the circulation of blood in response to sudden or intense changes in gravitational or centrifugal forces 19 labile blood pressure |
|
Anyone who writes about, or discusses, or benefits from my 1982 methods of treating chronic fatigue with exercise and general activity, or any derivation thereof, should show some respect to me for making it , possible, understandable, and safe, by calling them “The Banfield Principles“, and not give the false impression that they are their own idea, or someone else’s methods. Thank you. The Banfield Principles For Exercise Training and symptom management in the Chronic Fatigue Syndrome (the effort syndrome) First devised in 1976, & later modified between 1980 & 1983, and then, following some criticism 25 years later, in 2008, presented with more detail below. These principles could also be called guidelines, or protocols, and all modern methods of treating CFS with exercise have to be based on them, simply because I perfected them andit would be impossible to treat the problems safely or propeerly without them. Introduction
Patients who have the chronic fatigue syndrome need to understand that I actually have this ailment, and that, in many cases there is no cure, but that I am able to control the symptoms, so I know what I am talking about. Although I have developed a method of exercising consistently and within my own limits, i would never force anyone else to exercise if they don’t want to. I know how much trouble this ailment can be, and how difficult it is to manage, so I care about you. Getting rest when necessary, is a very useful method of treating the problem, but as a general rule, I find that a combination of rest and walking is beneficial. You should not feel guilty or angry if you don’t want to exercise so I can give you an example of the research program I developed in 1982. Many people made phone enquiries but were too tired, or too physically exhausted to attend classes. Some who started only stayed for one session, and some for several weeks. However, of those who trained in exercise classes each week, some remained at the same levels, some improved slightly, and one person appeared to return to normal levels. Exercise is not, and should not be compulsory, but it is something for you to consider and try if other methods aren’t helping. The following principles are based on what I did. The Principles 2. Some individuals may be too readily exhausted to exercise, and if they benefit from rest, they should rest. If they are able to exercise the exertion should be faster than standing still and slower than sprinting, and the level of starting should be determined by the individual, and the rate of improvement should be gradual. 3. If the individual is walking or training with other people they may be always passed by other participants or walking at the back of the pack. This should not be a deterrent but if it is then people with this ailment should train in groups where all participants are aware of the nature of the problem and the programme. (Exercise ability is proportional to aerobic capacity and the Effort syndrome involves an abnormally low aerobic capacity which varies from person to person). 4. Healthy people recognise that when they train fast they can often force themselves past any perceived limits of endurance with the expectation of getting a second wind that enables them to proceed in comfort. This is a common observation amongst marathon runners, but it may be nonexistent or ineffective in The Effort Syndrome and should not be relied upon. 5. While walking or jogging a sense of breathlessness can occur at irregular distances, sometimes after twenty yards, and then after the next fifty yards, and then again thirty yards further. This symptom can be relieved by taking two or three forced breaths each time without causing any problems. If these do not relieve the symptom, slow your pace, or stop if necessary, but sometimes these forced breathes may be occasionally necessary, even at rest. The breathlessness is probably due to inefficient function of the diaphragm (the main breathing muscle), and a forced inhalation expands the chest sideways and improves the oxygenation of the lungs which is deficient because of less downward movement of the diaphragm. 6. If distressing symptoms of palpitations, faintness, or dizziness occur at improved levels of exercise then return to a lower level, and improve gradually again later. 7. Faintness can be due to any factor which traps blood below the waist, especially if the blood vessels have been strained by many years of stooping which can result in a tendency of blood to pool in the blood vessels below the waist and reduce the efficiency of circulation. Therefore faintness may be induced by stooping, or leaning forwards, or by any factor which constricts the waist such as tight belts and girdles. Hence to prevent faintness those factors should be avoided. It is worth noting that 19th century women tended to faint because they wore very tight wasp-waisted whalebone corsets. They relieved the faint by loosening their corset laces, and by laying in a chaise-lounge, with their body horizontal, and their head and shoulders slightly elevated on the arm of the lounge. The faintness was relieved partly because the waist constriction was released, and partly because the gravitational load on the blood vessels was removed, and blood could therefore flow toward the head unimpeded. In fact fainting results in falling to the floor, and this is natures way of getting the body into the horizontal position so that blood can flow to the head and the person can recover. Additional notes on faintness: 1. Even snug fitting belts can cause problems because they restrict the free expansion and contraction of the abdomen which accompanies breathing, because that compresses the internal anatomy and impairs the downward movement of the diaphragm. 2. Faintness can also be due to wearing tight collars because they also reduce blood flow to the brain, so always wear the collars loose. 8. Faintness can also be due to the looseness of internal organs (visceroptosis) which move excessively when the body is subjected to gravitational or centrifugal forces. This movement can compress abdominal blood vessels and impair blood flow from the feet to the brain. The problem can be relieved by stabilising the body and contracting the abdominal muscles to minimise the movement of internal structures. 9. The effort syndrome has been called neurocirculatory asthenia because it features a weakness in the circulation of blood. This results in a tendency to faintness and dizziness because of an abnormal disturbance to blood flow in response to such things as sudden intense exertion, sudden loud noise, or sudden changes in gravitational or centrifugal forces. Hence the person may feel faint, or as if they are about to collapse when they suddenly sprint (e.g. when they hurry to catch a bus) or when they are exposed to sudden loud noise, or when they suddenly move from the laying to the standing position or when they ride in a lift. In order to deal with these it is useful to recognise that they are not natural responses, and that therefore the natural way of dealing with them is not effective. However in much the same way as riding a bicycle is an unnatural method of traveling which is different to walking, and can be learned through practice, the method of dealing with the symptoms of the effort syndrome can be learned. This essentially requires a mixture of periodic resting, and the practice of breathing deeply and regularly three or four times in order to relieve any symptoms when they occur, and repeated practice and experience makes this more effective. 10. The effort syndrome can be effectively managed by restricting lifestyle and exercise levels within particular limits so that the person gives the appearance of being in perfect health. In fact maintaining optimal fitness within those limits is useful in managing the condition. However this appearance of health is often misconstrued or misrepresented as being evidence that the person is in perfect health, and that they should be able to maintain any lifestyle and participate in any exercise that they wish, and they are accused faking. The fallacy of these accusations needs to be understood by the patient so that they are not coerced into going beyond their limits and bringing about a relapse of prolonged unremitting exhaustion. (which has some similarities to being on a overdose of coffee – The Kramer Syndrome – where rest, relaxation, and sleep are not easily attained, or effective in relieving the fatigue) |
The Banfield Principles continued: Specific methods for treating the Effort Syndrome
1.If rest is necessary then rest is the best treatment at that time 2. If walking is possible then walking is the best exercise 3. Any improvement in fitness levels should be gradual 4. Do not carry heavy weights when walking, especially in the early stages. 5. As a general guide avoid sprinting, especially if carrying weights. 6. Avoid anaerobic exercises such as weight lifting or forced movement against any form of resistance. 7. Set your own pace in exercise and do not be concerned with the improvement rates of other people because they may have a higher aerobic capacity. 8. Walk on flat ground, especially in the early stages when you are assessing your aerobic capacity. 9. As a general guide do not walk up steep hills until you understand your fitness limits, and then only do so if you think that it is practical and possible, and at a pace determined by your experience. 10. If you occasionally feel as if you are not getting enough air when you are walking or jogging, then take two or three forced deep breaths each time, and you should be able to continue. 1. If abruptly moving from the laying to the standing position makes you feel faint, then first move to the sitting position and then stand up slowly, and wait a second or two before walking. 2. If riding in a lift makes you feel as if you are about to faint, then avoid lifts and use escalators. If you need to use lifts then enter the lift and take three or four slow, deep breaths before the lift begins to rise, and again each time it slows to stop. 3. If you have to use lifts, then it is likely that your natural reflexes can adjust to the movement of lifts, but it will require more time than normal, and will require the practice of breathing techniques to reduce the effect of the gravitational forces which are involved in the lifts movement. 4. If traveling by aircraft makes you feel faint and distressed, then try the same treatment as specified above when the plane accelerates to take off or decelerates to land, or when it drops in an air pocket. 5. If riding on whirling sideshow rides causes you to feel faint and distressed then avoid them. 6 If you feel faint when you are a passenger in a car which is speeding around a curve in a country road, then brace your arms against the dashboard and contract your abdominal muscles to stabilize your body. Alternatively avoid such journeys, or ensure that you are the driver so that you can brace your arms against the steering wheel and can adjust the speed of the car according to the way your body is responding. 7. If you feel faint when your car is braking to stop at stop lights, then approach the lights slowly, and brake gradually, and take a few deep breaths before braking, and brace your arms against the steering wheel so that you do not slump forward as the car stops. 8. If you feel faint or dizzy when squatting down and leaning forward, then avoid activities which involve squatting, especially for prolonged periods of time. 9. If you feel faint when leaning toward a desk, the kitchen sink, or the washing machine, then move closer to the task so that you reduce the tendency to slump forward, and try to keep your back straight by bending at the hips instead of the midriff. 10. If you feel faint or dizzy in a crowded room or theatre then sit in an aisle seat so that you can leave if necessary, without disrupting other people. The faintness may have been due to the noise of the movie, or to high concentrations of CO2 which can accumulate in crowded areas. 11. If you are in a theatre and feel faint or experience palpitations when a crescendo of music is followed by a loud clashing sound (for the purpose of creating suspense), then take a few deep breaths to break the effect of the sound waves, or leave the theatre auditorium temporarily, until the symptom eases. 12. If you are tempted to sprint for some urgent reason, as when hurrying to catch a bus, then ensure that your increase in pace is modified and within the limits which you have learned from experience, or do not hurry at all. 13. If you feel faint it may be partly due to the fact that you are wearing tight belts, girdles, corsets, or collars which reduce blood flow to the brain, so loosen such garments, and lay down for a few minutes, preferable with your head and shoulders slightly elevated and your knees raised with your legs bent. As a preventive measure, never wear tight or constricting garments. For my YouTube video on the cause and treatment of faintness see here http://www.youtube.com/watch?v=Xs770_nwq6I See also this reference B.Biswal, P.Kunwar, B.H.Natelson (2011), Cerebral blood flow is reduced in chronic fatigue syndrome as assessed by arterial spin labeling, Journal of Neurological Science, Feb. 15, 2011, 301(1-2), 9-15. This is the result of the study of the cerebral blood flow (CBF) of 11 CFS patients compared to 10 age matched healthy controls . . . “The patients as a group had significantly lower global CBF than the controls. The reduction in CBF occurred across nearly every region assessed. Nine of the 11 patients showed these reductions compared to the average control data, while two patients showed actual increases relative to the controls. See here |
|
The measurement of the Effort Syndrome Introduction
|
|||||||||||||||||
|
The measurement of cardiovascular fitness in the Effort Syndrome The aerobic capacity in chronic fatigue patients is abnormally low and explains why they have a reduced capacity for exercise and are more easily exhausted than usual
The pulse rate increases according to the amount of effort being exerted. The relative increase varies from person to person and can be measured, and that measurement is referred to as their cardiovascular fitness, their aerobic capacity, or their physical working capacity (PWC 150). In one method of measurement each individual is required to sit on the seat of a stationary cycle while wires are attached to their chest by suction cups. The other ends of the wires are connected to a cardiograph machine. The person is then asked to peddle for a period of time, such as one minute, while there is no brake pressure on the wheel, and their pulse rate is monitored. They then have a similar period of rest and then start again after minimal pressure is applied to the brake, and then they have another minute of rest, during which time the load on the wheel is increased. This riding and resting proceeds several times and each time the load on the wheel is increased again. The researchers can then assess the results and draw a graph of the pulse rate which was recorded at each level of resistance, and use it to determine a scientifically accurate and reliable measurement of the level that is required to produce a pulse rate of 150 beats per minute. That level of resistance is known as their kilopon rating and gives an indication of cardiovascular fitness. When these experiments have been conducted on groups of people with the chronic fatigue syndrome there is always a percentage of them who have abnormally low levels and they are the ones who could be identified as having a type of cfs for which the term The Effort Syndrome is appropriate. As a guide for comparison an athlete would have a capacity of 1200 kilopons, and a person of average fitness 900 kilopons. Some people with cfs have readings below that of individuals who have other chronic illnesses, and for the purpose of consideration anyone with cfs who has a level below 500 kilopons could be regarded as having a sub-group of the condition for which the term The Effort Syndrome applies. The person can then participate in an exercise programme where they are required to train for one hour a day, three days per week for three months. Each sessioni includes walking or jogging with their pulse rate reaching 120 to 140 beats per minute for 20 minutes. There can also be 20 minutes of formalised aerobic, but non-weight bearing exercises, and 20 minutes of other physical but non-vigorous game activity. At the end of the three month training session a second ergometric test can be conducted to determine if the programme has resulted in any measurable improvement in cardiovascular fitness, and then a further three months training performed, and the test repeated again. This programme would determine the persons kilopon rating, and whether it improved with exercise or not, and if there was no further improvement at any stage it would also show their upper kilopon limit. Example result for patients who had persistent problems with fatigue 1. At outset zero kilopons, after three months 355 kilopons, after 6 months 355 kilopons. 2. At outset 260 kilopons, after three months 240 kilopons, after 6 months 250 kilopons. 3. At outset 325 kilopons, after three months 500 kilopons, after 6 months 540 kilopons. 4. At outset 375 kilopons, after three months 450 kilopons, after 6 months 780 kilopons. Note that in example 1 the measurement of zero resulted from the graph being drawn in the usual manner as a straight line, but a more precise reading can be achieved at the lower levels if the graph is drawn with a curve. The first level of zero was achieved peddling up to a maximum resistance of 150 kg, the second of 355 up to a maximum resistance of 450 kg and the third of 355 up to a maximum resistance of 750 kg indicating that measurable cardiovascular fitness had plateaud despite an increased ability to peddle against resistance. When I discussed these results with one research cardiologist I said that they were scientific evidence of a physical basis for persistent fatigue. He replied with a tone of resentment in his voice and said “No! that meant nothing!” I did scientifically prove that chronic fatigue was a real physical ailment, but for one reason or another some people don’t want to admit it.
More details about the research project and a graph showing results can be see here
|
|||||||||||||||||
|
The Aerobic Ceiling
|
|||||||||||||||||
|
The exertion crisis in the Effort Syndrome, and it’s management
There have been reports of recruits who have been required to carry heavy knapsacks and sprint along an obstacle course at army training camps, and as they increase their pace they suddenly collapse and they roll about the ground having spasms and fits. Their symptoms have been attributed to a fear of exercise or a sub-conscious fear of battle, and they have been deemed unfit for military duties for psychological reasons. However a closer study of these recruits reveals that many of them were known to have had the symptoms of an effort syndrome for many years previously in civilian life. It is most probable that these people had been managing their condition by limiting their activities until such time as joining the army and being required by their training officer to exceed their physical limits. There have been numerous attempts to cure the effort syndrome by using exercise programs which gradually improve physical fitness to normal levels, however the majority of those programs invariably failed. Some years ago I heard about a fitness program which was being conducted at an oval in the grounds of a mental hospital to treat patients who were suffering from fatigue, so I made some enquiries, and when I spoke to the psychiatrist who was organising the program I suggested that,if a physical method was being used to treat chronic fatigue then it was a bit incongruous to regard it as a mental illness , and he responded with embarrassed silence. Many people with chronic fatigue report that they feel physically distressed when they attempt to increase their level of exertion. The heart pounds with excessive force with each contraction, but when it expands again there is a sense that the heart muscle is weak and becoming more exhausted and may not have enough strength to contract again, so there is a sensation of an impending faint. This sensation is relieved when they reduce the pace of their jogging, so if they are asked or told to run faster than they feel capable of they simply drop out of the course. However some of them do, usually only once, exceed their limits, as for example, when being required to participate in a relay race, and the following symptoms occur as they rapidly increase their pace. Firstly their heart suddenly begins to pound and rock violently in their chest, and then all vision disappears and is replaced by a black visual field with thousands of small bright spots, like shooting stars, darting in all directions, and then the person feels faint, as if they are about to collapse. Then to avoid collapsing uncontrollably they lower themselves to the floor and crawl about on their hands and knees, feeling the continuing violent pounding of their heart for a minute or two, as well as an intense sense of hyperactivity, as if their bloodstream has been saturated with twenty cups of strong coffee, so that any restraint of movement causes distressing physical agitation, and a sensation that if they do restrict their movement they will lose consciousness. They therefore pace about restlessly on their hands and knees and they tell other people who come near them to help to keep away, and not to touch them or restrict their movement. They then have to reach for breath to get oxygen into their lungs to satisfy an intense air hunger, and they avoid talking because the exhaling of air to produce speech drains them of energy to the extremes of exhaustion. As they pace about on all fours the effort exhausts them so they have to rest, but after a few seconds the restraint of movement causes profound distress so they have to pace about again, and they continue in this alternating way for about 10 minutes. The symptoms then ease somewhat and it is possible for the person to carefully lift themselves onto a chair, but the effort exhausts them so they slump in the chair, but the slumping restricts their breathing so they have to sit upright. If that effort exhausts them they may have to move back to the floor again for a few more minutes of rest and slow pacing, and then they can lift themselves up into a chair again. After another 10 minutes or more their rapid pulse, and their breathlessness, and their sense of intense hyperactivity eases, and they can stand to walk.They will then have to intermittently rest and sleep and pace about slowly for about a week before resuming any exercise program, and then only at a lower level than was achieved before, and with a more gradual improvement regime, and they will be unlikely to ever exceed their own perceived limits again. They may ultimately achieve considerable improvements to their physical capacity but not be able to return to a normal level of fitness regardless of how frequently they train because there is probably an anatomical limit to their aerobic capacity. I have referred to the Exertion Crisis as Sudden Exertion Shock or Sprint Shock. M.B. (I wrote this item probably between 2007 and 2009, and it is based on my personal experience of exceeding my own limits in 1976 and on several occasions since, and on several research papers indicating these features with less detail. Research findings 1975-2011 confirming the effectiveness of my methods with more scientific evidence and proof of aerobic limits The description of the exertion crisis was based on my experience while participating in a standard exercise programme at the South Australian Institute for Fitness Research and Training in 1975. I was asked to design a research programme by the head of that institute in about 1982, and included methods of ensuring that the participants did not exceed their limits or have that experience, and measurements of aerobic capacity were taken at three monthly intervals as described in detail in other parts of this webpage – e.g. See here and here On 15th June 2011 I produced a YouTube video on the relation between breathing pattern and exercise can be seen here A video on scientific measurements by cfsks.com/media (www.cfsKnowledgeCenter.com & www.me-cfsCommunity.com) can be seen here In this video Dr. Nancy Klimas, MD, director of the CFS Clinic in Miami, explains that the measurements were for VO2 maximum, up to which the individuals physiology is able to supply enough oxygen and sugar to their body (within their aerobic capacity), and above which they exceed their aerobic capacity and go into anaerobic levels where there is not enough oxygen being delivered for their needs and they start experiencing fatigue. She then explains how an exercise programme can be designed to enable the person to stay within their limits. In a second video by the same organisation a patient explains how he uses the VO2 principles to stay within his aerobic capacity – to PACE himself – and stay within his exercise limits, which he found to be very useful and an excellent way of improving his health. See here |
|||||||||||||||||
|
|
|||||||||||||||||
|
Postural and visceroptosis induced hypotension and faintness
One possible explanation for the results of the tilts test is that some people with The Chronic Fatigue Syndrome, particularly those with The Effort Sydrome, have visceroptosis. In that case all of the major internal organs would be loosely suspended, and hence would be significantly movable in the abdomen. Therefore when the body is tilted the intenal organs would begin to slide and cause symptoms, until eventually they compress the major abdominal veins and reduce the blood flow returning from the feet to the heart, and hence reduce blood pressure, and induce the sense of faintness. (This sense of faintness can be quite different from normal faintness and may be very distressing to the patient.) The movement of the internal organs could be ascertained by doing x-rays at each phase of the tilt test. A similar symptom can occur when the patient moves suddenly from the laying to the standing position because the abdominal organs drop forcefully within the abdomen, but that can be prevented by first moving from the laying to the sitting position and then standing up slowly. By constrast when the person moves from the standing position to the laying position the abdominal organs slide toward the heart (like fluid inside a half-full bottle flows toward the cork when it is laid on its side), where the pressure can cause the symptom of palpitations. This symptom can be prevented by first moving to the sitting position and then laying down slowly onto three pillows which keep the head and shoulders slightly eleveated. After a few minutes two of the pillows can be removed. Similar symptoms can sometimes also occur during pregnancy because of the movement of the heavy pregnant womb which occurs when the woman changes position. For more information on visceroptosis see The Visceroptosis Webpage To view a diagram of sliding visceroptosis see the sliding visceroptosis diagram |

|
Levels above 5 are consistent with CFS and are associated with the Effort Syndrome |
0 | 5 |
10 |
| Non-fibrilla catabolism | |||
| Fibrilla catabolism |
|
“The urine often shows a white or pink-coloured deposit on standing, and there may be a movable kidney – this condition being, indeed, a well recognised cause of neurasthenia in women . . . True neurasthenia is purely a functional disease – i.e. there is nothing wrong with the machinery.” Reference: The Modern Family Doctor (1928) p.479-480. |
The measurement of chest width, depth, and sternum angles
There have been numerous observations that people with CFS often have thin and narrow chests, but other patients have normal or obese builds therefore it is possible that the thin chested physique may be more specific to The Effort Syndrome. This is because such a physique crowds the heart and lungs and alters their shape and the sharpness of the curves of the main arteries, and would probably influence cardiovascular function, as well as disposing to visceroptosis. Therefore the following measurements would probably be relevant.
1. Chest shape measurements
The severity of the spinal stoop, the narrowness of the chest, and the flatness of the chest could be measured directly by measuring the curve of the spine, the width of the chest, and the angle of the breastbone, but perhaps a better guide would be the measurement of the distance between the lower tip of the breastbone and the spine. These measurements may show that the smaller this distance, the more likely the incidence of The Effort Syndrome
2. Heart shape measurements
The shape of the heart may influence heart function, and in this respect the measurement of the length of the heart in relation to body height, and the width of the base of the heart may be relevant. A pyramid shaped heart of average height with a broad base may tend to be more stable in its function, whereas a bowling pin shaped heart which is tall and thin with a narrow base might have a greater tendency to unstable wobbling palpitations, and a more common association with The Effort Syndrome.
The measurement of the extent of visceroptosis
There have been numerous observations of a link between visceroptosis (the displacement of abdominal organs) and CFS but these associations have been dismissed because of some inconsistencies. However further studies may produce a more reliable link between visceroptosis and The Effort Syndrome, and the more significant the visceroptosis the more likely the association. The following suggested measurements could be made.
1. Minor visceroptosis with significant displacement of one abdominal organ.
2. Moderate visceroptosis with significant displacement of up to three abdominal organs,
3. Severe visceroptosis with obvious displacement of five or more abdominal organs, and with the base of the stomach extending below the navel.
For more information about visceroptosis see The Visceroptosis Webpage
|

|
The Chronic Accrual and Recurring Fatigue Syndrome
CARFS Webpage ©
|
The Frog in the Frypan (I think I made this comparison more than 30 years ago, but have just added it here again on 27-12-11) The symptom of fatigue in CFS is different from normal fatigue in two ways. 1. First of all it can increase so gradually over a period of many months that the person doesn’t notice. 2. Secondly, when the person does decide to stop all activities and get complete rest, with the expectation of recovering within a day or two, they don’t. The fatigue tends to persist for two or three months at the same level where it is difficult to do anything but the mildest of physical activity. This is somewhat similar to the concept about the frog and the frypan. If you place a frog in a very hot frypan it will feel the pain immediately and jump out without harm. However, if you place it in a cold frypan and gradually warm it up, by the time the frog realises that it is hot, it will be too late to get out. If you told the frog what was going to happen it would jump out as soon as it felt warm. Although I still have the problem of CFS, I haven’t developed severe uncontrollable fatigue since, because if the symptom increases, I notice it, and take steps to ensure that it doesn’t progress any further. |
The Runaway Freight Train Syndrome 11-7-06
The problem of chronic fatigue syndrome is difficult for the general population to understand because it is not seen as being much more than the problem of normal fatigue. Therefore I will try to explain it by making a comparison with a runaway train.
While the train is traveling along a flat plain, it can slowed down by applying the brakes, and then when it comes to a small downhill section it will speed up again under the influence of gravity, but it can be slowed by applying the brakes again, and that process of speeding up and slowing down can be sustained for 100 miles, and is equivalent to the way people go about their lives, and rest or sleep when necessary to maintain a healthy sense of well being throughout 100 years of life.
However, when a train begins to descend a steep mountain track it may initially speed up and then be slowed by applying the brakes, time and time again, until the brakes begin to weaken, or the steepness of the mountain increases, or the slipperiness of the track worsens, in which case the brakes won’t work effectively so that the train never actually quite returns to its standard speed. As the steepness increases and the brakes become less effective, the train continues to accelerate even if the brakes are constantly and fully applied. The train won’t be able to stop until it reaches the bottom of the mountain and then travels a very long distance across the flat plain below.
That is what the chronic fatigue syndrome is like. As long as a moderate lifestyle is maintained there does not seem to be a problem, but if fatigue occurs, and if nothing is done about it in the early stages, it will reach a degree of severity where normal amounts of rest or sleep will not quite restore normal energy levels. In such cases the fatigue will subtly, and almost unnoticeably get worse until it is uncontrollable, and then months or years of rest may be required. Furthermore, it may not be possible to achieve full recovery, and with the basic problem remaining, the fatigue is likely to recur for various reasons at various intervals of time and require long term rest to recover from.
Telling a person that “we all get fatigued” and “all you need is rest” is not going to be effective, any more than a manager from the station emergency department is going to help the driver of a runaway train which is cascading uncontrollably down a mountain by saying to the driver “have you thought of using the brakes”. M.B.
|
New Definition 19-11-04 modified 1-8-05 Chronic Accruing and Recurring Fatigue Syndrome (CARFS) The Chronic Accruing and Recurring Fatigue Syndrome (CARFS) is a type of “chronic fatigue syndrome” in which the patient appears to be healthy but where regular activity which is sustained for weeks or months may result in an insidious accrual of fatigue until it becomes profound and extreme and impels the person to take complete rest and several months to recover, and where, upon the resumption of regular activity the process repeats itself. This may be due to a weakness in the main abdominal vein called the vena cava so that systemic blood flow becomes insufficient and disturbed and causes apparant compensatory responses of the cardiovascular, neurological, energy, or exercise functions that appear to be regulatory disorders and it prduces subtle and accruing systemic overreactions. The accruing fatigue possibly results from the weakness of the vein or from systemic overreactions and have formerly been misdiagnosed or misrepresented as a series of nervous or mental breakdowns). Defined 21-5-03 and redefined 1-8-05 |
||||||||
|
Other former titles for the condition which provide clues to its nature
The dysregulated sleep pattern I noted that the condtion had been called Vasoregulatory asthenia many years ago, and it prompted me to draw a comparison with the sleep problem not simply being due to a lack of sleep, but due to a disorder os sleep regulation. Nowadays that concept would be described as a “Dysregulated Circadian Rhythm“. |
“Effort Intolerance” is so commonly encountered in cases of the Chronic Fatigue Syndrome that it should be classified as the hallmark symptom of a specific condition which has formerly called The Effort Syndrome, and any condition which does not include that feature should be recognised as being different. Such other forms of chronic fatigue may involve only tiredness and should be referred to as sleep disorders, or where the tiredness is due to a sense of sadness then the problem would be referred to as depression.
There are many people with “Effort Intolerance” who are not always tired, and are rarely or never depressed, so unless the condition is defined separately there will always be confusion in understanding or defining the problem.
Within the category of “Effort Intolerance” there are nevertheless other fatigue related symptoms which may overlap the symptoms of sleep disorders and depression, and there are a collection of other symptoms which accompany the condition which is why it produces confusion in diagnosis and why it is called a “Syndrome” (the word syndrome is derived from the Greek origins “syn” which means “with” and “dramein” which means “to run”, where symptoms often run together or characteristically occur as a collection in the one ailment).
Symptoms related to fatigue include “Effort Intolerance” where mild levels of exertion are possible but high levels are not, i.e. the ability to walk at a casual pace for many miles, and to do mild exercise regularly and often where only moderate improvements in fitness are possible, and the capacity for normal levels of fitness or to engage in strenuous exertion is never achieved (also breathing symptoms, faintness, and dizziness occur, but are more likely to be associated with exertion). Other fatigue related symptoms include the tendency for tiredness during the day, the tendency for fatigue to accrue over a period of weeks or months of sustained normal activity, and the tendency to develop over fatigue or exhaustion which is not relieved in the normal way by short periods or rest, such as hours, weeks, or months. This could be referred to as the Chronic Accruing and Recurring Fatigue Syndrome or CARFS, and it is most likely that CARFS and Effort Intolerance are seperate features of the same problem with the same cause.
Other symptoms in the syndrome include lower left and right sided chest pains, sometimes stabbing or lancing in nature, cramping chest pains occurring on the extreme left and right side of the chest, a form of breathlessness which occurs periodically as a brief difficulty breathing in, as if breathing inwards until a limit is reached so that a full breath cannot be achieved, faintness (with or whithout actual fainting), dizziness, upper-abdominal pain, aches in the back in the region of the kidneys, neck ache and shoulder pain usually occurring on one side, and lower back ache or pain. Many of those symptoms are related to postural changes, such as postural hypotension (orthostatic hypotension – postural low blood pressure) which causes a sense of faintness and dizziness when moving from the laying to the standing position. That type of faintness is often associated with unstable blood pressure (called labile blood pressure) where there are fluctuations between low and high blood pressure, and these can be evident as a persons body is moved up down or sideways on a tilt table where they sometimes report experiencing very distressing symptoms of faintness or impending collapse. .
People with the chronic fatigue syndrome are often but not always characterised by a particular physique which includes a thin build, a stooped upper spine, forward arching of the lower spine, sideways curvature of the spine, and, a long, narrow, or flat chest. M.B.
There has been much presumed and said about effort intolerance in The Chronic Fatigue Syndrome being a consequence of a fear of exercise, but this is because doctors have been writing such stuff based on the absence of laboratory evidence, and their reluctance to believe what they have been told by patients. To really understand this problem, in the absence of scientific proof, would involve doctors actually experiencing this problem themselves, but when that happens their own colleagues have been sceptical. In an attempt to redress this misunderstanding I will give a contrasting account of symptoms related to extreme sport in healthy people, and the symptoms occurring in CFS exertion crises.
Introduction: An example of my experience with sport before I developed CFS
See also here
When I was 15 years old I was a member of a lacrosse team. When the original coach left, another coach took his place, but was often too busy with other duties to attend training sessions or matches, and after losing more than a dozen games in a row one captain after another stopped attending. Ultimately, the remaining members of the team held a meeting to select an on field captain. I was late for the meeting and when I walked through the door I was told that I had been elected unanimously because I reliably attended games and was the oldest. Despite my protests at not wanting the job, I was made captain anyway. We lost more than another 10 games when we came to play the top team in the high school league.
We rolled up with 6 players (mostly small) against the opposition of 10 (mostly taller) which had several spare players accompanying them, and, rather than abandoning the game, they gave us some of their spare players as substitutes. I won most of the opening plays against the state centreman by using a trick or two. Nevertheless, it wasn’t long before we were losing by about 20 goals to 1, so I had a backman take my place in the centre with instructions to swing the ball in my direction in the outfield. The other members of the team were instructed to distract the opposition when I got the ball because I was going to hog it in an attempt to get a goal on my own, for the hell of it. The ball came in my direction as planned, and after scraping it from the ground I was being attacked by 2 opponents so I ran back toward their goal, and as they were still following me, I ran behind the goal, and then across the back of the field. I then ran forward and made a full on charge at the captain, who was much larger than I was, and although I was not going to ram him I did have him bluffed. At the last moment, I dug my sprigs into the ground and angled left, leaving the captain behind. I was then being attacked from the front by two taller backmen, so I ran to the outfield and along the boundary, with about 4 players positioning themselves to stop me getting through to the goals. I then raised my net and ran directly for the goals. When one of their backmen came charging toward me I feigned a throw, and turned my back, and swiveled my head and gave a facial expression as if I was mystified about where the ball went. This temporarily had all of the opposition looking in the direction of my throw, and at that moment I ran straight for the goal again. It was then obvious to those players that I still had the ball, so one of the backman brought his heavy stick up and over my head and belted it down. It bounced off the side of my head and grazed my ear, and rammed into my shoulder. I then turned my back, and then angled my way straight toward the goal, with only two backmen pursuing me. I increased my pace, and left them just far enough behind to be ineffective at stopping me, I then had only the goaly to deal with. He was the biggest goaly in the league, and seemed to occupy the entire frontage of the goal, so I raised my net to aim the ball straight between his eyes, in a bluff aimed at getting him out of my way. Of course I didn’t want to put him in hospital, so my next move was to pirouette and swing the ball backwards with a scooping action under his feet. By that time the goaly had thrown his stick into the air and had run away laughing. I assumed that he thought that anyone who had ran through every member of the best team in the league deserved a goal just for the joke of it. In any event, the ball rolled slowly across the unguarded line, making the score about 20 goals to 2. In the meantime, I was still rotating in the pirouette with a lot of momentum, and I stumbled forward for about 15 yards before losing balance and falling to the ground. In the process of evading all ten members of that team I probably ran, mostly flat out, a distance of more than 200 yards. My heart was pounding, I was gasping for breath, and I felt the taste of blood welling up in my throat, but that wasn’t an entirely unusual thing for me to experience in sport. After about a minute I staggered to my feet, and could hear a lot of raucous cheering and laughing, and while still struggling to get enough energy to speak I yelled out to my other team members, “OK fellas, we’ve got them worried, now let’s finish them off”.It was probably only two or three minutes before I had made my way back to the centre to continue play. When the game ended about 20 minutes later we had been massacred 49 goals to 3.
The point of this description is to give some insight into the fact that I played a lot of sport, mostly for the fun of it, and anyone who thinks or says that I am, or was afraid of exercise, has lost the plot.
Some more examples of sport before I had chronic fatigue syndrome.
Exercise Training in The Chronic Fatigue Syndrome – A Biography I played a lot of sport as a teenager, sometimes on cold and rainy mornings on ovals that were 3 inches deep in mud and water, and I ran in hurdle events and the mile, and up and down hills and valleys in cross country races. I was also involved in a private gymnastics club where, on a typical night I would arrive at 7 p.m. and assist with moving heavy wooden springboards and vaulting horses from their storage shed into the hall. The next 4 hours would involve warm up sessions, which sometimes included tossing a 5 kg medicine ball back and forth 50 times, followed by training sessions which included 50 or more somersaults off the floor, or off springboards, or teeterboards, or over the 4 and 5 foot vaulting horses, and the evening would end with team relays, or a game of indoor soccer or volley ball, after which the equipment would be carried back to the shed, finishing at 11 p.m. On summer weekends we would often go down to the beach and somersault down sand hills and go swimming, and diving or somersaulting off jetties.
In my late teens I obtained 3 scholarships to study Group Work at The Institute of Technology. The first was from The National Fitness Council of Australia, the second was from the State Government Department of Community Welfare, and the third, which I accepted, was from the Commonwealth Government. I completed the course of subjects which included individual, group, and social psychology, and politics, and I had interests in leadership methods, creativity, and conformity.
Later, in my role as leader of the gymnastics club, I would typically stand in front and demonstrate 20 push ups, 30 toe touches, and 40 side stretches etc, for the class to follow. However, there were occasions when parents would advise me that their child had a health problem such as asthma, which could benefit from exercise, but they would show concern that too much strain could be a problem for them. I dealt with this by advising the child to do the same exercises, but not to worry about trying to keep up the same pace. I also instructed the group not to criticise him, as that would prompt him to try too hard for his own good and would discourage him from continuing.
When I was about 22 I had a very large steak and vegetable meal for tea, and 10 minutes later walked into the gym and flipped into a hand spring, and felt something rip inside my belly. The incident seemed uneventful but about 2 months later I started getting an ache in my belly whenever I leaned toward my desk in my job as a clerk. This ache gradually became worse and was eventually accompanied by various other problems such a faintness, breathlessness, or dizziness whenever I leaned toward the desk.
Eventually some of those problems also affected me in the gym when for the first time in my life, exertion was giving me problems.
Examples after I developed the chronic fatigue syndrome
I first noticed it when, on one occasion, I demonstrated a round off back somersault, and when my feet thudded to a stab landing, a thousand stars splayed across my eyes, and I felt dizzy, and faint, as if I might collapse.
A few months later I was getting a pounding heart each time I lifted my left foot, and then my right foot off the ground, and I was confined to laying down a lot because of the effort of walking.
My doctor was unable to explain these symptoms and they were getting progressively worse so I resigned from the gymnastics club, and soon after that I resigned from work and began reading a medical dictionary at the rate of one or two words a day until I found that my symptoms were consistent with an ailment called Da Costa’s syndrome. (It would now be called the chronic fatigue syndrome).
In order to prevent being crippled by abdominal pain which occurred soon after I started leaning toward a desk to read or write I would read for five to ten minutes and then lay on my back on the lounge room carpet and think while staring at the ceiling for most of the day. (Thinking never caused me any pain at all).
As my health had previously deteriorated gradually over a period of about 3 years, I also decided to participate in a fitness programme with the view to gradually improving my fitness and recovering full health in a year or two. I therefore enrolled in a course at The South Australian Institute For Fitness Research and Training.
My initial fitness was measured and found to be zero, as compared to a friend of mine who had an average fitness of 900, and an athlete level of 1200. Part of the programme involved jogging, and typically I could only jog slowly for about 20 yards before struggling for breath and having to rest. For example in a group of 50 people I would be running last around an oval, and for a while I had a companion. He was 40 years old, overweight and asthmatic and I told him not to worry about leaving me at the back alone, and that he should run ahead and catch up with the group which he did. As the group out lapped me two 50 year old men ran together and one said, in a voice loud enough for me to hear, “we have an excuse for being unfit because we are 50 and have spent years smoking; we are not like the youth of today (meaning me) who are unfit because of laziness”.
After 3 months training my fitness level rose to 350 so I increased the number of days I trained to 4 per week. On one occasion the instructor ran some relay races and I ran as fast as I could, but was not much help to the team, and then we were required to squat down and place a 5 kg medicine ball between our knees and frog hop to the end of the hall and back. After 10 yards my heart began to beat violently and I fell to the floor and crawled around on all fours feeling faint and dizzy and on the verge of collapse for about 10 minutes. It took me a week to recover from that 10 yard run. On another occasion we left the hall and ran through the streets for a change. After about 300 yards all the other runners were so far ahead that they had gone around street corners and were out of sight so I ran alone for about 20 minutes until returning to the hall 10 minutes behind everyone else. After 6 months my fitness was measured again but it was still 350 despite improvements in my speed, strength, and endurance on the ergometric cycle. (fitness level was measured by graphing pulse rate over load). During the ninth month I was training 6 nights per week but I threw knee cartilage and had to stop.
A couple of years later I was invited to attend the gymnastics club annual camp and while there I was invited to participate in a game of soccer. When I tried to run and get the ball I would get the same problem with pulse rate and faintness and have to stop and simply get the ball only if it passed within a few feet of where I was standing.
I had been making detailed observations and studying each of the symptoms, including the fatigue, for about four years when I finally concluded that most of them could be attributed to leaning forward, and wrote the first account of The Posture Theory as an essay called The Matter of Framework. The fatigue was due to postural pressure on the air in the chest which blocked blood flow and stretched the veins below, similar to the way in which a garter blocks blood flow in the leg and causes varicose veins below the garter line. However unlike varicose veins which show up on the legs, the enlargement of the main veins in the abdomen, or the whole system may not be visibly evident, but something was impairing the normal blood flow through the body and that was my estimate of the causes of exercise problems and fatigue.
Shortly after that I discussed my ideas with the head of the Fitness Institute and he suggested that I run a research programme to study the problem in more detail. I was aware from the medical literature that the general view was that these patients could not or would no train and that their reluctance to participate in exercise programmes was generally attributed to a fear of exercise. Other researchers were treating the patients as if they were physically sound and expecting them to train in normal programmes with healthy people. However, I knew that the pressure to conform would make the fatigued patients run faster than their limits and cause problems, so it did not surprise me that all of them refused to run, or dropped out of the courses before results could be achieved.
Therefore in order for a programme to succeed and provide improvements in health and meaningful data it would need to be designed so that fatigued patients were in a group of their own under instructions to walk or run at their own pace within their own limits, and not to be concerned about how fast others were going.
The first 3 month course involved about 20 people with 6 remaining at the end. By the end of the third course about 80 people had been medically assessed and more than 12 were still training with some continuing for the entire 9 months, and one person participated in a 6 mile marathon. The fitness levels at the outset had examples at the level of 100 and 300, but there were also some at 700 or 1100 and that data confused me until some years later when I suddenly realised that there were different types of chronic fatigue syndrome (for example the low measurements would relate to exercise disorders, and the high measurements to sleep disorders)
Unfortunately the writing of the data involved desk work which was aggravating my abdominal pain so when I was asked to increase the programme to include 200 participants I stopped.
My health returned to tolerable levels after about 10 years but I never fully recovered.
For example, every summer I would go to the beach and run about 10 paces along the sand and then hop step into a hand spring, and when I landed abruptly with my back arched and my arms outstretched I felt a rip followed by a gnawing ache in my belly. I did that once every summer for at least 5 years, always with the same response and have never had a medical explanation for it. Similarly, one day I was digging in the garden and the spade struck a rock under the dirt. The sudden jolt caused a pain in my midriff which persisted for 3 months and was accompanied by severe constipation for that time. Also whenever doctors prodded my belly with their finger during medical investigations I have always felt pain when that same spot is struck, and on some occasions it has persisted for a week after.
In those early years I decided to build a carport and pergola around my house. I would start digging with a post hole digger at 9.a.m. After 10 minutes the hole would be 1 foot deep but I would be breathless and dizzy and have to stop and rest for half an hour. At 11 a.m. I would start again and 10 minutes later when the hole was 18 inches deep I would have to stop and rest again. By mid afternoon through several digging sessions I was able to complete 1 and a half holes 3 feet deep. At 4 p.m. my neighbour would return from his full days work and dig 3 or 4 holes in an hour without having to stop and rest.
Specific Examples of exercise limitations in the chronic fatigue syndrome
Also there were times when I would go to town by bus, and sometimes I would be late so I would have to walk fast or jog to get to the bus stop on time. On one occasion I had to walk briskly, and was at my limit when I saw the bus passing across the end of the street. I then walked faster until I got around the corner and could see the last passenger getting on, so I ran, and my heart began to pound violently so I had to stop. I watched the bus driver looking at me as if I was too lazy to run and then he drove off in disgust and I had to wait in the cold and rain for the next bus.
I kept feeling generally healthier as time passed so from time to time I would try to run and could go quite fast for short periods of time but there was always a problem with symptoms if I didn’t keep within reasonable limits. However sometimes I got caught in situations where I was motivated to ignore those limits. For example I often go walking, sometimes up and down hills, but on one occasion I was asked to join some bush walkers. It was difficult enough to keep up the pace in the early stages but then the leader turned left up a steep hill. I puffed and panted to get to the first tree about 10 yards up and after reaching the second tree little old ladies and old men with walking sticks started to stream past me. By the time I got to the top of the hill every one else was relaxing and chatting and eating their sandwiches or having a cup of tea, and I was trying to hide my breathlessness and look as if If had gone slow because of loose shoelaces. A few years later I was able to walk quite briskly up several flights of stairs so I would do so as a form of regular exercise, instead of getting the lift.
Some time after that I was walking up and down hills for exercise when I met a friend who asked me to follow him down a track to see some native flowers. When we got to the bottom there was only one way out – up – and it was steep. He kept his normal pace on the way up but after about 10 yards I was puffing and panting and my heart was pounding so I had to grab hold of a tree trunk for support. My friend looked at me from 50 yards ahead and his dog came bounding down and licked me in the face as if in a reassuring manner and then went bounding up again. The dog would disappear and come bounding back several times before I reached the top gasping for breath.
In summary, the condition that I have been discussing is nowadays called The Chronic Fatigue Syndrome. I believe that the term was first used overseas before 1975, but I cannot recall when it came into general use in Australia, or when I first became aware of it. However I have been able to establish that it is measurable, that its severity varies from person to person, that it involves an exercise disorder and, or a sleep disorder, and that the condition generally responds favorably to appropriately designed exercise programmes and may even, in some cases be cured. However in other cases, despite participating in exercise programmes which would make an average person extremely fit, and despite improvements in the general feeling of well being, there will remain a persistent limitation until the exact anatomical cause can be confirmed and cured. M.A.Banfield
See the Banfield Principles for Exercise Training, and symptom management in a type of Chronic Fatigue Syndrome called the Effort Syndrome here
Conclusion
As any one who reads these accounts can clearly see, there is a lot of difference between the physical response to exercise in healthy people, and the response in people with The Chronic fatigue syndrome. M.B.
Quotes from other authors
Caughey J.L. Jr. M.D.(April 1939) Cardiovascular Neuroses: A Review. Psychosomatic MedicineVol.1, No.2, p.311-324 . . . The typical patient with the ‘effort syndrome’ was “‘‘never allowed‘ to take part in competitive sports” and has felt inferior physically to others of his own age”. . . “They never learned to keep on when the going was hard” . . . during the exercise test . . . “the response is no more dependent on the amount of exertion as it is than on the emotional reaction he has, the fear that he has that the test will injure seriously his already weakened heart” (end of quote)
Paul Wood O.B.E. (1950) Diseases of the Heart and Circulation 2nd edition, Eyre & Spottiswood, London p.943 . . . From chapter XX111 about patients with the ‘effort syndrome’ . . . “They are timid children far too dependent on maternal protection. At school, kindly doctors and soft mothers protect them from the hazards of football, swimming, and the gymnasium. It is probable that predisposition to psychoneurosis is mainly hereditary, but early environmental factors, such as domestic strife, insecurity, suppression, and maternal coddling, play their part . . . Fear of football and fear of swimming are common in childhood, and may precipitate anxiety.” (end of quote)
The second reference was by Paul Wood, and it had a major influence on attitudes toward the condition, changing the general view that it was an ‘effort syndrome’ to an ‘anxiety disorder’ that has prevailed until today.
To give you some indication of how misleading it is, I can say that you have just read my description of how I participated in sport when I was a teenager. I would play in the cold and the wet, and the rain, on an oval 3 inches deep in water and mud, without my spectacles, and without a helmet, for the fun of it. I also attended swimming classes for several years at the local beaches and was a good swimmer, and would go canoeing in the sea and rowing in rivers, and dive off jetties, and do summersaults down sand hills. I never had a fear of swimming or sport, and I was a gymnastics instructor for five years and a gymnastics leader for an additional five years, and I could easily summersault from springboards over 5 foot high vaulting horses, and I was often the first to arrive at the gym and the last to leave. I have had natural aptitude for some sports and none for others, and have been among the best and worst in teams in some games, and have had all of the cuts and bruises that occur in anyone who plays sport for more than 10 years.
2012
I found an article published on the website of the Hunter-Hopkins Center, P.A. by Charles Lapp, and Laura Black Called “Relapses and Flare: Dealing with relapses and flares” .
The chronic nature of the CFS and how to adapt to it
I have seen many definitions of the Chronic fatigue syndrome but they all include the main symptoms of chest pains, palpitations, breathlessness, faintness and fatigue – and problems with exertion.
However, those symptoms are often presented in texts or lists but are not mentioned in order of prominence, but are generally included in random order on a list of 10 or more which include muscle soreness, swollen lymph glands, abdominal pains etc. Nevertheless, the main ones are always there.
It is also said that the diagnosis is not given unless the person has had the symptoms for at least six months or more. It is also generally said or implied that there are various cures available. However, while it does appear that some people who have had a mild version of the condition for a short time do recover, the vast majority continue to have the symptoms recurring throughout their life.
I have personally interviewed and met people who have had the problem for much more than 20 years, and although they have adapted well to their limitations, they still have problems with fatigue, and there are research studies which followed the lives of patients for 20 years or more, and provide similar information.
It has also been generally advised to reassure patients by telling them that it is not a permanent problem, or that one form of therapy has been proven effective as a cure, or that a cure is imminent, and of course, some people use the the ‘victim blaming’ tactic of blaming the failure of treatment on the patient.
Whilst reassurance, is, of course, a sensible thing to do, it has to be said that after a few years the doctor simply ceases to have any credibility, and the patients don’t believe it any more, and further reassurance is a complete waste of time.
The false reassurance certainly doesn’t make the chronic, incurable problem go away.
It is relevant for me to now mention that some years ago I became interested in Dale Carnegies book called “How to win friends and influence people”, and it contained an item about teenagers who become paraplegics after a car accident. He wanted to know how they dealt with the news that they would never walk again, and would always be stuck in a wheel chair. He was told that at an early stage the doctor has the difficult responsibility of giving the bad news, and that false reassurance, and false promises of a cure was a waste of time because it would just delay the teenagers process of adapting to the changes in their lives. He was also told that for the first 12 months the teenagers go through periods of denial, and then anger, and then fear, and then depression, but that sooner or later they accept their fate, and get used to the idea without being miserable. From what I can recall he gave the example of boys who were going through a shopping centre in their wheelchairs and laughing amongst themselves about the “wheel deficient” shoppers.
As far as the chronic fatigue syndrome is concerned, many patients worry about their symptoms, and about fifty percent are depressed after about five years, and some go mad or commit suicide. I suspect that it is due to false reassurance, and false hope that there is some sort of cure coming up the next day, with the next pill, or the next research discovery. However it never happens so the patient is always dealing with disappointment, and consequently never accepts or adapts to the chronic nature of their condition emotionally.
Many people with chronic fatigue would probably be much better off if they accepted their limitations, and led their lives within them.
The problem isn’t exactly that simple, but it is also not impossible to deal with.
Expecting, or demanding the CFS patient to do the impossible
There are many illnesses which are not properly understood and cannot be cured, so regardless of what type of treatment is given the person will have to learn how to relieve the symptoms as effectively as possible and live with it. Typical of those is asthma, or diabetes.The asthma involves allergies, so the person needs to avoid such things as environmental pollens that trigger the breathlessness, and diabetes involves abnormal responses to various foods that affect insulin levels, so they have to be careful with their diet, and may have to have daily injections of insulin to maintain stable health. In the case of the chronic fatigue syndrome it is necessary to make changes to lifestyle to reduce the reduce the demands for energy etc.
However, there are many doctors who don’t want to admit that they don’t understand the problem and have failed to cure it, or that their choice of treatment has failed, so they pass the burden of proof onto the patient who is uneducated and never read a medical book in their life, and they blame them them for the failure of treatment by saying such things as this . . . “The “patient” is a “therapeutic failure“.
The issue is this . . . If the doctor can’t cure it, and if the best scientific researchers in the world can’t cure it, and if the best treatments can’t cure it, then it is unreasonable and unethical to expect the patient to cure it.
The Banfield Principles for CFS activities
If you can walk one step at a time for long enough you canwalk a mile, or ten.
If you can lift one kilogram at a time for long enough you can move a ton.
If you can write half a page of text per day for long enough you can write a thousand page book in six years.
I am not recommending it, but merely pointing out to any nitwit who says I’m lazy, that it is exactly how I did it, and the only way it was ever going to be possible.
The Chronic Fatigue Syndrome
The Banfield Proof
of Physical Cause ©
Posture, pregnancy, corsets, viruses, chemical exposure and
Postural & Mechanical Hypotension
As a cause of tiredness, sleep and exercise disorders, and other related symptoms.
Anyone who still disputes that CFS has a real physical basis has the onus of proof to scientifucally explain the symptoms described on this webpage in some other way.
8-2-2005
Removing The Confusion
|
From my research of years and decades ago to modern ideas and methods When I developed the theory that poor posture and physique were the cause of chronic fatigue, I tested the idea by looking at other patients, and noticed that not all of them had those features, so I assumed that it was a ‘disposing’ factor that made the problem more likely, but later, when I discussed my ideas, other people who had different opinions about cause would become argumentative or hostile, and I would have to respond to their comments, or politely refrain from saying anything to keep them calm. However, one day I was at a South Australian ME/CFS seminar when many people were arguing about psychological, neurological, and chemical causes etc, when I drew the conclusion that there must be several causes, and several types of the condition. Nowadays most top researchers recognise that there are different types and are trying to determine the difference, but no-one quotes me, presumably because I just wrote my own books or this website, and they only quote from articles published in “research journals”. I developed the idea of multiple causes about 20 years ago, and wrote the article below, in 2005. Recently, on 14-10-2-13, Tom Kindlon provided a link to a YouTube video which Dr. Kenny De Meirier discussed the different subgroups of CFS. See below . . . |
Before discussing this type of chronic fatigue it is necessary to clear up some confusing aspects of the subject, otherwise people who have other types of the condition will be sceptical and argumentative at the outset and will not even bother to examine the facts, and doctors who do not understand the difference between normal tiredness and the most severe types of chronic fatigue will continue to say to their patients “What are you complaining for; we all get tired sometimes”.
There are two types of normal fatigue
|
Tiredness which results from lack of sleep |
Physical exhaustion and breathlessness which results from extreme exertion such as completing a marathon |
There are two types of chronic fatigue
|
Tiredness which is unrelated to a lack of sleep and can occur at any time of the day or night in a manner which is abnormal, irregular, and, or excessive.. |
Physical exhaustion, palpitations, breathlessness, faintness, and dizziness which occurs in response to the slightest exertion, or is out of proportion to the amount of exercise. e.g excessive symptoms occur in response to sudden efforts, lifting, running, or climbing. |
There are two other confusing aspects to consider
| 1. The severity of each problem varies from person to person so it can be difficult to distinguish normal fatigue from chronic fatigue (although in severe case this is obvious to a patient who has formerly been healthy and athletic and can make the comparison) | 2. Some people with chronic fatigue have a only sleep problems (a sleep disorder) and some have predominantly a difficulty with exercise (an exertion disorder) but often there is a mixture and overlap of the tiredness and the problem with physical exercise. |
Two Opposite Pyschological Possibilities; Is it Cause
or Response
|
1. Cause? It has been suggested that anxiety makes the blood pressure rise and the heart beat faster, and that the abnormal response to exertion is due to a fear of exercise. It has also been suggested that depressed people get tired. For these reasons anxiety, fear and depression have been proposed as causes of CFS symptoms. The failure to find evidence of cause has it diagnosed as being “all in the mind” and the failure to measure it’s severity has it diagnosed as “trivial”, or as an abnormal and unwarrented concern about the sort of normal fatigue which normal people would not complain about. |
2. Response? It has been observed that patients with CFS experience distressing cardiac symptoms during exertion and refuse to participate in exercise programmes, or are very reluctant to join in, and when they do most of them quit within the first week. The patients who may have been former athletes have to give up their sport. The patients also report that a variety of symptoms including frequent tiredness during the day, makes it difficult for them to stay awake and concentrate and remember, so they have to restrict their employment and social activities. Their doctors cannot diagnose the problem, measure it, or cure it , and give the impression that they do not understand it, so the patients become anxious and depressed about their health and their future. The cause of the chronic fatigue, as in some types of sleep disorder, is sometimes found and the tiredness is cured, and the patients return to their former lifestyle and cease being depressed. |
| 1. Cause: It has been argued that anxiety, depression, and suicide are so common in CFS that it must have a psychological cause. (Some doctors believe that 100% of CFS patients are suffering from anxiety so they call it Anxiety State, and others believe that 100% are depressed so they call it a depressive condition. However the medical literature refers to many CFS patients who are not suffering from anxiety or depression). | 2. Response: If consideration was given to CFS as being a physical illness, then the the associated data would make it a greater cause of anxiety, depression, and suicide that any other 10 illnesses combined. |
Three Outcomes for chronic fatigue
| 1. Temporary Fatigue; Some people experience an infectious illness where they have a cough for several weeks. They recover from the cough, but continue to suffer from fatigue for 2 or 3 more weeks, and then they recover from the fatigue and return to normal health without any treatment being necessary. |
2. Chronic Fatigue which responds to treatment; Some people stay out late all night at night clubs or casinos, and others are shift workers, which makes them tired all day, and if they change their lifestyle the tiredness is relieved. Other people have back pain or insomnia which keeps them awake at night and makes them tired during the day, and if those problems can be relieved and they get a good nights sleep, the problem is solved. Some people have chronic fatigue for many years until one day a medical test reveals the cause, such as sleep apnea, which can be treated by surgically removing a flap of skin at the top of the throat which has been falling back and blocking the airways when the person lays on their back to sleep at night. After the surgery, the airways are clear and the person can breath properly at night, so their sleep is not interrupted, and so they stop being tired all day and return to normal health. Some people appear to be afraid of the normal symptoms of exercise, and if, and when they participate in exercise programmes, they become accustomed to the symptoms and their fitness improves and they return to normal health. |
3. Chronic Fatigue which does not respond to treatment; Some people have chronic fatigue for many years, and despite having many medical tests there is no evidence of the cause, so there is no effective evidence based treatment. Some people participate in exercise programmes to improve their fitness, and while they may continue training and improve their frequency and duration of activity, and while they gain measurable improvements in their strength and aerobic capacity, and some relief of symptoms, they do not return to normal levels of fitness, and continue to have problems with exercise and fatigue. |
(Some causes may produce a common fault – damage to the vena cava? and, or postural hypotension)
The Vena Cava syndrome
Throughout history chronic fatigue has been a common aliment, and it has been given more than 100 different labels. There have also been more than 100 different suggestions about cause, and as a result there have been many heated and hostile arguments about whose idea is correct and whose is wrong. However, I, and others have suggested that there may be many different types, and several different causes, which could mean that none of the people in any particular argument might be wrong. The might just be talking about a different type or cause. It would seem that the best thing to do would be to present some sort of united study of the ailment, or group of ailments.
| Poor posture |
When a person with a stooped spine and a flat chest leans toward a desk they can compress the air in their chest to produce a pneumatic tourniquet which blocks blood flow from the feet to the brain in a way that is similar to a tourniquet on the arm which blocks blood flow to the hand and makes it go numb. Blocking blood flow through the chest also puts downward pressure on the blood in the main vein of the abdomen and could stretch its wall and eventually make it weak so that the person has a chronically impaired upward blood flow. Chronically weak blood flow to the chambers of the heart would impair a persons capacity for exercise, and also result in a chronically impaired blood flow to the brain which gives the person chronic problems with concentration, memory, faintness, and tiredness. This is evident from various tests which show an apparent inability of the body to regulate or maintain normal blood flow. A feature of this problem is postural hypotension where a person feels faint if they stand up too suddenly. The sudden and extra weight of blood in the abdominal vein would make it stretch so that it takes a few extra seconds for the blood to fill it before reaching the heart, and hence the slight delay in blood reaching the brain causes temporary faintness. The main abdominal vein is the vena cava, but all of the veins below the midriff might be involved. The chronic fatigue syndrome includes all of those symptoms, so postural compression of the chest and stretching of the vena cava, or all of the veins below the chest, may be the cause of the condition. |
| Pregnancy |
During pregnancy the enlarging womb gets heavier and compresses the abdominal veins and many pregnant women experience faintness and fatigue. This usually ceases after giving birth and the womb returns to its normal size and weight, but some women continue to suffer post natal fatigue which has been called post natal depression |
| Genetics/ Heredity |
Some people appear to be born with the chronic fatigue syndrome, or have one or more parents with the condition. It is common in children, and some adults have had it for so long, and it occurred so gradually that they don’t know when it started. |
| Tight Corsets |
Nineteenth century women wore tight waisted whalebone corsets which compressed their abdominal veins and they were known to faint in response to the heat, or exertion, or slight frights. They relieved their faint by unlacing the corset and laying flat which allowed blood to flow freely to their brains. |
| Shock waves/ electrocution |
Soldiers exposed to bombing attacks sometimes develop shell shock because of shockwaves that pass through their bodies. Sometimes the shockwave makes them temporarily or permanently deaf or blind and sometimes it leaves them temporarily or permanently exhausted. That is called battle fatigue which is another name for chronic fatigue. The shockwaves can sometimes cause the human abdomen to explode, and it may also have a violent effect on the blood in the vena cava and weaken the walls of the vein. |
| Excessive physical exertion, marathons, world record attempts etc |
Some marathon runners, and athletes who attempt world records develop chronic fatigue. This may be due the excessive exercise or effort without adequate rest and sleep etc. and to the prolonged and excessive strain on the blood vessels, and the vena cava. In some cases it is called The Overtraining Syndrome (OTS). Some nineteenth century soldiers developed chronic fatigue after marching for days or weeks, up and down hills, in cold and wet weather with poor food, and infectious illnesses such as malaria or typhoid, which caused fevers and dehydration. They couldn’t keep up the pace of the other soldiers but kept going until they became faint and exhausted and fell out of line. Although they recovered from the infection a few months later, they continued to have chronic problems with exertion and fatigue. |
| Overwork |
Excessive physical work and long hours of work without rest can cause chronic fatigue. In the nineteenth century some coal miners who were required to shovel a particular tonnage of coal each day developed chronic fatigue so the British government set up an organisation called The Industrial Fatigue Board. Some authors have attributed the chronic fatigue to overwork. The excessive strain could damage the vena cava in the same way as world record attempts. i.e. Normal exertion causes normal fatigue which the body can recover from, but excessive strain or exertion for excessive periods of time, may exceed the bodies limits, and causes so much fatigue that the body cannot recover to it’s former capacities. |
|
Viruses |
There are examples of factories or villages where a severe viral infection spread through most of the individuals. They recovered from the flu symptoms in a few weeks, but some of them continued to suffer from fatigue for many years after. That is an example of post-viral fatigue. Perhaps some viruses can damage the walls of the vena cava. Examples of that typed of CFS are The Royal Free diseases in the staff of a London hospital, Tapanui flu in New Zealand, and Icelandic disease etc |
| Chemical exposure |
Some poisons, or pesticides may be able to damage the vena cava which may explain why some people report suffering from chronic fatigue which can be traced back to exposure to toxic chemicals such as pesticides, or those associated with factory chemical spills, or the toxic gases of war (mustard gas in WW1, Agent Orange in the Vietnam War, and toxic oil fumes etc in the Gulf War). Glue sniffing can cause fatigue, and medically prescribed drugs such as barbiturates can cause or aggravate postural hypotension. |
| Abnormality in the nervous system |
There have been various suggestions that chronic fatigue may due to a disorder of the central nervous system, where the symptoms are due to an abnormality in that part of the brain which controls automatic functions such as pulse rate, breathing rate, and blood pressure etc. Some have suggested that the problem may be caused by a virus damaging that part of the brain. Others have suggested that there is nothing physically wrong with the brain, but that constant anxiety is stimulating that part of the brain to increase the affect on the body. However, there is also the possibility that it is just the affect, and not the cause of the problem. For example, if there is an unknown abnormality in another part of the body which causes various malfunctions, the abnormal activity in the brain may be a reflex response to it. |
| 48 interviews on cause |
While researching this ailment I interviewed 48 people and asked each person to tell me what they thought the cause was. There answers can be seen here. |
Many people experience postural hypotension temporarily and make a full recovery. For example, some teenagers grow rapidly and their lower spine sways forward as they become thinner and taller. They generally develop postural hypotension, probably because the sway back presses on the abdominal veins, or because the rapid growth of the spine stretches those veins and impairs the flow of blood to the heart. This gives them a tendency to feel faint when they rise from the laying to the standing position, particularly when they get out of bed each morning. However as they reach adulthood their body fills out and the feature of postural hypotension ceases to be a problem. Pregnant women also tend to develop postural hypotension because the weight of the enlarging womb drags their spine forward, and also because it sits heavily on the lower abdominal veins. The tendency to faint varies throughout pregnancy depending on the weight and position of the womb, and although the symptom usually ceases after giving birth, sometimes the symptom persists in a chronic way.
There are various suggestions about the cause of postural hypotension including the ideas that it is due to hormonal factors, or a disorder of the nervous system, and it is a chicken or the egg matter. i.e. Do the hormones or the nervous system abnormalities cause the weakness in blood flow, or does the weakness in blood flow put the hormonal or nervous systems into compensatory action.
Nevertheless there is evidence that mechanical factors cause impairment to blood flow, and it is likely that the persistent or repetitive pooling of excessive amounts of blood in the abdominal veins stretches and damages them. That would increase their capacity permanently and result in a chronic tendency to postural hypotension where the responses of the hormonal and nervous systems would be secondary.
Impairment of blood flow to the heart would produce firstly, problems during vigourous exertion (effort intolerance – where the person refuses to exert themselves suddenly or viguourously because it brings on abnormal and distressing symptoms of rapid palpitations, faintness, and dizziness), and secondly, problems with weakness in blood flow to the brain resulting in abnormal tiredness. Postural hypotension, effort intolerance, and chronic abnormal tiredness are features of The Chronic Fatigue Syndrome, but not all people with CFS have evidence of postural hypotension, so the idea that the hypotension is the cause has been the subject of debate.
Nevertheless there are differences in the severity of CFS between individuals, and in the life history of patients. Sometimes CFS appears to be genetic, and other times it appears to have a very gradual and insidious origin, but typically the first bout of fatigue can be traced back to an incident, such as pregnancy, a viral illness, or chemical exposure. In such cases the original experience reached a peak of fatigue which impelled the person to take rest for months or years, during which time they gradually recovered but remained permanently impaired to a lesser degree. There are also typical examples where there were years of minor fatigue, interspersed with brief periods of more severe fatigue. It is therefore likely that the postural hypotension is a chronic latent feature which is only evident during severe cases or with the relapses.
In severe cases of CFS the symptoms tend to be worse and more numerous and varied. One of the prominent symptoms is postural hypotension and the obvious indication of weakness in blood flow is the tendency to feel faint when moving from the laying to standing position, especially when getting out of bed in the morning when patients report the they have to stand up very slowly to avoid feeling faint. Other less common observations are the sense of faintness which patients report when they lean toward a desk to write, or when they lean toward the washing machine to drag clothes out, or when they lean toward an ironing board to iron clothes, or when they lean toward the kitchen sink to wash dishes. They may also feel faint and dizzy if they squat down and lean forward to clean low windows, or when they apply the brakes suddenly while driving a car and their body is thrown forward, or when they are a passenger in a car which speeds around a curve in a country road and throws their body sideways, or when they are sitting in the chair of a rotating amusement ride at a carnival. Many patients report feeling an extremely distressing form of faintness when their body is being moved up and down and sideways at all angles on a tilt table while having some types of x-ray. All of those factors have a mechanical effect on the body, and the response is often immediate, so the condition is clearly mechanical hypotension.
If the veins below the midriff, or all veins leading to the heart, i.e. all of the venous system was stretched and had greater capacity, then there would be a tendency for blood to pool excessively in response to any obstruction to blood flow. Therefore if a person stood up suddenly the blood would pool below the waist in response to gravity increasing the weight of the blood, and it would tend to pool below the midriff if the person leaned forward and compressed the air in their chest, and it would pool in the legs if a woman was pregnant and the heavy womb was compressing the abdominal veins behind or the pelvic veins below, and it would pool in the extreme outer parts of the venous system if the body was subjected to any type of centrifugal force.
Therefore there is evidence that mechanical factors can cause damage to the walls of the veins to produce postural hypotension which is in turn responsible for the symptoms of chronic fatigue (effort intolerance and tiredness), However, those veins would have some resilience, and therefore some ability to recover, which would explain variations in the severity of the condition at its onset, and variations in the severity between individuals, and variations in the recovery times, and it would also explain the chronic nature of some cases, and the fluctuations in the course of the condition in others.
Any medical research group or patient organisation could easily test this theory and determine the presence or not of proof of a physical basis for CFS by using the following methodology.
1. Gathering 200 patients who report the symptoms of CFS
2. Testing the aerobic capacity of those patients using ergometric cycles and cardiographs
3. Selecting the 100 patients with the lowest aerobic capacity
4. Attaching blood pressure monitoring equipment and cardiograph leads to the patients.
5. Measuring the resulting data while the patient is being tilted up and down at various angles and rotated at various speeds on a tilt table.
6. Documenting the results for public review.
2. That the results are predictable
3. That the results are consistent
4. That the experiment is performed independently by several investigators
5. That the results are different from those of a control group (of healthy patients)
1. When some people refer to the chronic fatigue syndrome as trivial they are not basing their statement on a scientific measurement but are merely giving an opinion (a reckless and irresponsible guess)
2. When people say that the condition has a psychological cause they are not suggesting that every patient with CFS is anxious or depressed because that is simply not true. They are basing the idea on the absence of absolute proof of physical cause and typically arguing “if it is not evident on physical tests it must be psychological, otherwise there is no other explanation”. Of course they are not looking very hard for other explanations or they would have found countless possibilities.
3. The suggestions on this web page can be tested by anyone who wishes to do so and some matters are worth considering in relation to postural hypotension (a type of faintness which is brought about by standing up too suddenly or by other similar acts which are entirely physical and mechanical).
(a) If pregnant women feel faint because of a fear of pregnancy and childbirth then why do they only feel faint at particular periods of the pregnancy, and if it is not due to the weight of the womb pressing on abdominal veins then why is it aggravated when they lay on their back and relieved when they lay on their side.
(b) Why so some women during and after pregnancy, feel faint and giddy and get exhausted when they lean toward a sink, or an ironing board, and why does their heart pound when they lay on their back at night when they go to bed.
(c) If nineteenth century women felt faint because of multiple fears then why did their symptoms ease when they loosened the laces of their corsets and layed down on a chaise lounge.
(d) If patients are afraid of having their x-ray taken on a tilt table then whey aren’t they afraid of having a plain chest x-ray while standing, and if they are afraid of tilt tables then why do they only feel faint when the tilt table is moving, and why does the faintness vary in intensity with the angle of the table, and the speed of the movement, and why do they stop feeling faint when the tilt table stops moving.
(e) If patients feel faint during some postural movements then why do they feel faint when slumping and leaning forwards and not when leaning backwards
(f) If the faintness is not due to mechanical factors and, or, weakness in the walls of veins, then what is the cause.
4. If the patients are afraid of exercise, why aren’t they afraid to walk, and if they can move at a measured or gradual pace why do they have problems with sprinting, and if they can walk on flat land or up slight hills slowly, why can’t they walk up steep slopes, and why is it that some of them were former athletes who never had any problems with any type of exertion, and why do some of them voluntarily participate in experimental exercise programmes and attempt to cure their health problems by improving their fitness.
5. Why do their hearts pump less blood during and after exercise compared with healthy people (do their veins stretch excessively in response to exercise and reduce the volume of blood returning to the heart chambers, and does that make the heart beat faster and more powerfully than normal in order to draw the same amount of blood up to its chambers each minute during vigorous exertion?).
6. Why do CFS patients have a measurably low earobic capacity and why does it remain low despite participating in exercise programmes.
7. If the cause of CFS is not physical then why do patients have abnormal breathing patterns during exertion (breathing becomes shallower, oxygen consumption is lower, and blood lactate concentration is higher), and why do they experience an elevated pulse rate for a prolonged period after exertio.
8. Why do they have poor breath holding capacity and an intolerance for CO2 and to wearing gas masks.
9. Why do they complain of aerobic distress when a cardiograph belt is strapped tightly to their chest but not when it is loosely strapped
10. If the symptoms above are not more likely to affect people with thin and stooped physiques who have long, narrow and flat chests then why was a life sized portrait of such a person painted by Ian Tillard and put on permanent display in the museum of the Post-Graduate Medical School of London (with reference to the Effort Syndrome). A photo of this portrait can be seen on page 941 of the book entitled Diseases of the Heart and Circulation by Paul Wood, published by Eyre & Spottiswoode in London 1956.
11.If the problem only effects timid softly spoken patients who are anxious, afraid of exercise, and depressed, then how can it be explained that some of the patients have formerly been confident athletes, and show no signs of anxiety or depression, and may be confident public speakers, while others show anger and hostility toward their own doctors (as reported in the medical literature).
Scientific proof of the tilt table method
Regarding my suggestions that tilt table test could be used as a means of testing for CFS, one of the main symptoms is faintness when standing up suddenly, which is also called orthostatic intolerance. The tilt table test is now being used as a method of testing for orthostaitic intolerance, so the method has been scientifically confirmed as correct. See here http://www.dizziness-and-balance.com/testing/tilttabletest.html
I was also referring to postural Valsalva’s maneuvre as a cause, and the laboratory use as a diagnosis which is now verified in the same website article.
Note that all of the references are recent from 1999 to 2009, compared to my suggestions of the relevance of tilt tables and symptoms from the 1970’s.This is one of the modern references; Kurbaan, A. S., A. C. Franzen, et al. (1999). “Usefulness of tilt test-induced patterns of heart rate and blood pressure using a two-stage protocol with glyceryl trinitrate provocation in patients with syncope of unknown origin.” Am J Cardiol 84(6): 665-70.
See also here http://www.gregpage.com/oiandd.html
When making a decision about the nature of an ailment it is not just a matter of accepting the only explanation available but of considering various possibilities and deciding the best for now.
In that regard the ideas of a psychological cause are based on a medical theory rather than objective fact
For example when consulting a doctor the patient may be told that there is no evidence of disease on an x-ray so the condition cannot be phyically based and must therefore be due to anxiety, and then, when the patient says that they are not anxious the doctor may believe that he is lying, or faking, or is suffering from sub-conscious anxiety, or does not know their own mind, or is out of touch with reality or is denying the presence of a psychological cause because of some presumed shame which the patient feels in relation to admitting to having a mental rather than a physical illness. All of those ideas seem plausible but are simply not valid for the following good reasons.
1. Many patients say that their symptoms could not be caused by anxiety simply because they are not anxious and the symptoms often exist in the complete absence of anxiety, and when other people suggest the presence of sub-conscious anxiety they are regarded as being disrespectful and annoying. Nobody likes being accused of being a liar or of not knowing their own mind and hostility toward such suggestions is perfectly normal
2. The reason patients say that their symptoms must have a physical basis is because they occur in response to physical, rather than emotional events. For example the symptoms are made worse by physical exertion, and higher levels of exertion are almost exclusively likely to bring on symptoms which are not evident at rest, or with mild exertion. Secondly the symptoms such as fainting are brought on by physical, not mental activities such as leaning or stooping or squatting, and by participating in activities which involve centrifugal forces, such as riding on swirling carnival wheels. Patients are not going to believe that those symptoms have a psychological cause no matter how many slick arguments are presented to convince them, simply because nobody is that gullible.
When deciding whether the symptoms of CFS are real or not, or physical or not, it is necessary to consider all the facts, not just opinions.
I would not be so arrogant as to expect anyone to believe what I said about this condition simply on the basis of my opinion, and no-one else should expect the public to be that mindless and gullible. It is a matter of making a decision on the basis of the facts, and that can only be done when all possibilities are explored, not just one.
1. That people with chronic fatigue are complaining about the sort of normal fatigue which an ordinary person would not be bothered by.
2. That chronic fatigue is a brand new condition of modern times
3. That the chronic fatigue syndrome is a rare condition
4. That people with CFS refuse to participate in exercise programmes because they are afraid of exercise, and that they could cure their condition if only they could overcome their fear of exercise and improve their fitness.
4a. That people with CFS are tired because of a lack of exercise and poor physical fitness.
4b. That if they simply forced themselves to ignore the symptoms they could exercise like everyone else
5. That people with CFS did not play sport as children or teenagers and are afraid of competitive sport.
6. That people with CFS are afraid of heart disease, and don’t know the difference between CFS and heart disease
7. That people with CFS are anxious or depressed about something obvious or subconscious.
8. That thinking positive and ignoring fatigue will enable the person to continue with the same normal lifestyle as anyone else.
9. That people with CFS are abnormally introspective and pay too much notice to the bodies normal function and misinterpret the normal beating of the pulse and normal functions of breathing and digestion as abnormal, and that they don’t know enough about medicine to recognise the difference between normal and abnormal body processes.
When I attempted to learn about the cause of the health problems of Robert Louis Stevenson I found that some biographers described him as an heroic adventurer who sailed the high and stormy seas and toured the world despite suffering from the plagues of tuberculosis, pneumonia, typhoid, and malaria which killed millions of his contemporaries. Other biographers described him as a whinging, sympathy seeking hypochondriac who was troubled by deep seated psychological problems and emotional insecurities that dated back to his early childhood.
That is an example of how a personality is determined by the individual but an interpretation is determined by others.
I have no particular interest in talking about my own personality other than to say that it compares favourably according to my observations of the world. The comments are made on this webpage because it is popularly believed that all people with chronic fatigue have anxious and troubled minds where anxiety is the cause of their symptoms, and that their reluctance to exercise is due to a fear of exercise, and that they complain excessively about trivial illness in an attempt to get sympathy, and that they would not know how to cope with a serious illness if they had one, and I do not believe that to be true.
I have survived more than 100 illnesses and injuries. For example 10 years ago I had bladder surgery and complications included several bouts of bladder blockage which was more painful than the pain of kidney stones, and that was followed by the cystitis of urinary infections. A specialist told me that blood tests and a CAT scan revealed that my body was riddled with incurable cancer and that I would probably be dead in 2 months. I walked about with post operative bladder ache for 8 months. About a year later I had further bladder surgery during a hospital staff strike. I underwent surgery while suffering from untreated high blood pressure and came out diagnosed by ultrasound as having a strained and enlarged heart and incurable high blood pressure and was advised to avoid strenuous exercise and take anti hypertensive drugs for the rest of my life. After learning about post-operative procedures during the previous surgery I recovered from the second bladder operation in a month. Since then I have had several other major problems including angina symptoms which I treated with a disciplined vegetarian diet rather than having bypass surgery. The symptoms subsided gradually over a 6 month period but I did not recover fully until another 18 months had passed. I also tried to cure the cancer with a 6 week fruit juice only diet. After 4 weeks I became exhausted so I ate some food but that gave me food poisoning and I was unable to eat for another week because of severe nausea and vomiting. Some time after that I had surgery to remove a 5 cm cancerous tumour from my neck, and the following day I walked for 2 kilometers. Shortly after that I started CHOP chemotherapy where I lived like a hermit for 6 months to avoid contagious infections as my immune system was depleted. 18 months later I had more surgery to remove a 10 cm cancerous tumour which was partially blocking my left kidney. That surgery left a 12 cm scar across the left side of my abdomen, and 5 days later I walked at least 5 kilometers down the beach. About a month later I started DHAP chemotherapy and that was followed by a stem cell transplant. Three doctors tried to convince me to use a self administering morphine machine to control pain and advised me that 90% of patients did so for a fortnight. I only had one morphine injection on the first day and declined the offer of the machine. Some other patients had very little nausea but the surgery and chemo left me ill and nauseas for 10 months, followed by another year of poor appetite. I then contracted a coughing virus which lasted for 6 weeks during which time I was bedridden for a month and my doctor advised me to get an ambulance and go to hospital where I spent a week with recurrent fevers and sweats, and was on tablets and a drip to offset the effects of dehydration, and oxygen to help me breath. The virus could not be detected or identified by blood tests.
By contrast I have met a 70 year old man who told me that he never had a sick day in his life, and I know of at least two people who have not had a days sickness of any significance in 20 years.
I am not afraid of spiders or snakes, and I am not afraid of sharks but am sensible enough to avoid the ocean and swim in pools and sometimes do so in those which are 20 feet deep. I am not afraid of public speaking which is reported as being the commonest fear which affects 90% of the population. I am not afraid of exercise and I am not afraid of disease, or death. I find it difficult to take life seriously and I often tell jokes and laugh a lot.
However, I have seen billionaire corporate criminals who live in mansions and float about on multi-million dollar yachts and cry and beg for sympathy on public television, and others who carry worry beads and look miserable and spend time in psychiatric hospitals and ultimately commit suicide after being charged with corporate crimes, and I have seen media personalities and politicians succumb to severe depression after their promising and prosperous careers were stifled, sometimes by their own folly, and I have seen movie stars who have had leading roles in 100 movies or plays who say that they had stage fright when they were young and still get stage fright every time they walk on stage 50 years later. I have seen sporting champions, Olympic athletes and mountain climbing adventurers talk about how they had one illness which threatened their activity and their life, and they have described it as the greatest challenge that they have ever had to deal with. M.B.
The Chronic Post – Q Fever Fatigue Syndrome
Query-fever on ABC TV
About 30 years ago I had health problems which were becoming progressively worse until they were seriously interfering with my capacity to do anything, including work. My doctor was unable to find evidence of disease regardless how bad the symptoms became, and the treatment was ineffective, so I eventually applied for sick leave, followed by recreation leave, but the symptoms weren’t relieved despite the rest, so I then applied for 12 months leave without pay in the hope of recovering. Ultimately I was left with no choice but to get more leave, or to resign and go on a pension, which would have amounted to 40% of my salary. However, I was then referred to a psychiatrist who asked me a lot of irrelevant questions, and then an administrative officer said that I would have to go back to work and work hard or be sacked.
I was advised by a Trade Union official to challenge the position but my health was so poor that I decided to resign, rather than go through the harassment of trying to convince any one that I had health problems when I had no medical evidence to support my claim.
During those early stages I also overcame boredom by listening to radio, and then turned to ABC radio because of their reputed attitude about proper use of the English Language, which might improve my ability to understand medical text. I heard a lot of doctors making statements in the name of medical science which were rash assumptions, tripe, or lies, so I became a talk back caller.
I frequently criticized doctors with ranting tirades, but the announcers had a discriminatory attitude toward doctors and treated their statements as the infallible truths of educated men, and treated people like me as ignorant uneducated people who weren’t qualified enough to give credible criticism, and who had trivial and mental rather than real problems, and didn’t know their own minds, or were simpletons who didn’t understand the complexities of disease.
I was often restricted in the number of times I could speak on radio ( to once per fortnight for two minutes under rigorous and almost vindictive cross examination), yet doctors would talk on radio for 15 minutes three times a week and be free to speak any ridiculous tripe they wanted to without question.
I adopted the tactic of using false names and addresses to get on radio more frequently.
Nowadays most of those doctors and radio announcers have died or have retired early with very healthy bank accounts.
It therefore entertained me to watch the ABC TV show Landline, on Sunday 27-11-05 when an ABC radio announcer – Kendall Jackson, from Port Pirie, reported her experience with Q-fever.
After suffering from some headaches, and thinking that they might be migraines, and then having really severe night sweats which saturated her nightwear, and then hot and cold spells, she thought that “something was majorly wrong” with her and that she was going “insane” so she consulted her doctor who diagnosed the flu.
Some time later she was doing a report about Q-fever in the local community and noticed that the people who she interviewed were describing similar symptoms to those that she had experienced
She then reconsulted her doctor and he confirmed that it was highly possible that her problem had been Q-fever.
The diagnosis of Q-fever is an abbreviation of “Query Fever”, because, when it was first discovered in Australia in the 1930’s its nature was a complete mystery – there was a query, or doubt about it, but since then it has been found to be present in almost every county in the world
Kendall Jackson was later interviewed on ABC TV show Landline, and as part of their investigation into Q-fever they contacted.
the Australian expert on the disease, Professor Barrie Marmion, who said that Q-fever is contracted from the droplets of moisture which enter the air from the placenta of infected cows during the birth process, and Kendall Jackson had been to a cattle yard just prior to her illness, for only 20 minutes. The condition can also be contracted from contact with infected sheep or goats, and typically affects people involved in the meat industry such as auctioneers, shearers, truckies, farmers, and of course “even rural journalists”.
Kendall Jackson also learned that there is sometimes a relapse of symptoms during pregnancy, and as a woman who had been pregnant, and who intended to have two more children that is an important thing to know.
Included in the Landline report were aspects of the money, and politics, and intrigue of the problem
Q-fever involves flu like symptoms such as headaches, and joint pains – hence the common misdiagnosis of the flu. The condition is usually temporary – just like the flu is usually temporary and over in a few weeks, but it has been only recently discovered that in 8-10% of cases the condition leaves a state of chronic fatigue. In particular, in the 1980’s while doing vaccine trials in Adelaide abattoirs, Professor Marmion found people who had previously contracted the condition “and they hadn’t got over it and they were lethargic and they really couldn’t cope with exercise which they normally achieved easily, and so on, and there were very few localising physical signs, except this general disturbance of various body systems”. >
One patient reported that he contracted the ailment while working on the slaughter floor as a meat inspector. He initially felt unwell and dizzy when one of his co-workers suggested that he see the factory nurse who told him that his blood pressure was extremely low. Since then he has had headaches and joint pains, and memory problems which were so bad that sometimes he couldn’t remember his own phone number. He also had sleep problems. During the first year of his ailment he would suddenly feel as if he was melting into the earth as he fell into a deep sleep at any unpredictable time. His wife said that his sleeps were so deep that she was scared that he was dead, or would never wake up. He felt that eventually he would get over it. but the problem persisted and he had to leave work. Eventually, After a battle with an insurance company he managed to get compensation payments equivalent to 75% of his former salary.
Of course that is where the politics of medical opinion arises – in the cost of disease to the meat industry.
The meat industry has a liability to pay for the cost of occupational illness, and Q-fever is a clear case of that.
They deal with this liability by having a policy of providing free Q-fever immunisation injection to all employees, to prevent the problem, with their policy summed up as “no jab, no job”. More than 85,000 doses of vaccine were given in a five year period.
Such a policy keeps the employees healthy, and saves the employer money – it suits everyone.
However, the 300 or more cases per year of temporary Q-fever cost the industry 1.3 million dollars per annum, but the cost of the chronic cases can be up to one million dollars per worker.
For that reason representatives of the meat industry are “nervous about discussing it” (it might create a rush of costly compensation claims), and reporter Prue Adams found that all attempts to interview the meat industry officials was met with refusal. They said that they didn’t want to because they might “become the target of common law claims”. . .”And compensation for Q-fever certainly has the potential to blow out “. . . “It’s big money”.
I would like to congratulate the Landline TV show for their informative programme.
The ABC Landline programme has given a good account of the cause, nature, prognosis, economics, politics, and intrigue of a “Previously Undetectable and Unknown Illness” – The Chronic Q-Fever Fatigue Syndrome, which is stereotypical of other types of Chronic Fatigue Syndrome, which has multiple causes, including Post Viral Chronic Fatigue Syndrome – i.e. conditions which are still the subject of much query, question, doubt, debate, politics, and intrigue – with suggestions that the conditions do not exist.
As Professor Barrie Marmion stated “I think that we badly need, for instance a decent diagnostic test for post-Q fever fatigue syndrome”.
|
Nowadays Q fever is known to be caused by a bacterium called Coxiella Burnetti. It is highly infectious and can survive in dust or soil for a year or more. Animals which breath in the dust become infected and although they show no symptoms they become carriers of the disease. The infected animals spread the disease to humans who come in contact with their urine, feces, milk, or blood, or who breath in the dust etc. It has an incubation period of 4 weeks and usually lasts for 10 days. The symptoms include fever, muscle pain, headaches, sweats, coughing, and fatigue. It’s antibodies are evident in blood tests and it is now treated with antibiotics such as tetracycline, but a small percentage of cases become chronic and are difficult to cure. Vaccines can prevent the problem. Reference – http://www.abc.net.au/health/library/qfever_ff.htm |
|
|
The Medical History of The Chronic Fatigue Syndrome and Stomach Ulcers
In 1975 Many researchers regarded chronic stomach ulcers and chronic fatigue as psychosomatic disorders for ‘sound scientific reasons’.
They observed that the lining of the stomach went pink when patients were subjected to stress, and it was said to be scientifically impossible for bacteria to cause ulcers because the stomach acid would destroy them.
They could not find any scientific evidence of organic disease in patients with chronic fatigue, and claimed that the patients were ill, only because they believed they were ill.
1995
In 1995 two Australian doctors, Robin Warren and Barry Marshall, were curing 95% of stomach ulcers with a 1 week dose of antibiotics, and chronic fatigue was officially recognised as a real medical condition by the Astralian Medical Association.
1975-1995
Between 1975 and 1995 patients were told to ignore their pain and fatigue and continue to work despite their pain. (Go back to work and work hard or be sacked). Many were forced to resign without compensation, superannuation entitlements, or pensions, and lived in poverty on unemployment benefits. Tens of thousands of them died from medically prescribed overdoses of Valium or barbiturates, or became depressed, went mad, or committed suicide.
2005
The Australian doctors who developed the antibiotic treatment for stomach ulcers were given The Nobel Prize For Medicine and said that there was a great deal of resistance from other doctors who refused to believe that it was not a psychosomatic disorder.
Some doctors still believe (or pretend to believe) that chronic fatigue is just normal tiredness. Their science is flawed or false or fake. (All talk and no cure).
The cost of disease to the national economy is the real hidden reason for blaming patients for disease. Nobody in authority considers the economic ruin of patients.
Consider this, the Nobel Prize winning doctors said (jokingly) that it is difficult to study stomach ulcers nowadays because they have become rare. Consider the number of ulcer patients who have been cured, and no longer complain of pain, and what changes that has brought to their life. Consider what would happen if doctors developed a real cure for the chronic fatigue syndrome. M.B.
About the author of this web page
(added on 2-11-05)
This section contains a brief biography of my experience with chronic fatigue and exercise
In the process I had the opportunity to discuss my own results with a research cardiologist (fitness readings from zero to 350 and plateauing) and I asked him if that was convincing scientific evidence of my condition being real and physical. The exact words in his blunt reply were astonishing and given in a resentful tone of voice; he said “No! that means nothing!!!” I got the impression that he was jealous of a non-doctor making a credible scientific discovery and proving some old theories wrong, but I wasn’t trying to prove anything. My objective was to solve my own problems, and offending doctors was just creating more problems.
Also I must say that I had courteous relations with most of the staff and doctors who were co-operating with me in the research, and because of my role as co-ordinator, I had access to the premises on a regular basis. However when I wanted to access my own file out of curiosity about the medical opinion given about me, I was advised that it was not standard practice to give non-doctors permission to read them. Nevertheless, I made a point of waiting until the staff were out, and went into the file room and read my own records. Within the text were the typed words “This man is a hopeless hypochondriac”. This made me furious so I stormed out of the building telling everyone in sight that they were all useless idiots. After calming down I apologised for my outburst, as most of them were not responsible for the remarks. In the meantime I decided that I could only rely on myself if I wanted to get any useful understanding of the problem.
(Regarding the doctor who diagnosed “hopeless hypochondriac” – When I first met him I was suffering from dozens of symptoms, including breathing difficulties, faintness, and dizziness, and my heart was pounding violently in response to the slightest exertion. I vaguely recall having difficulty walking from my car to the Institute building, and then I found it difficult to get up the stairs to the medical room on the first floor, and then the slight effort of riding the ergometric cycle produced a fitness reading of zero. I was also withdrawing from a high dose of barbiturates, and decided to study medicine myself because my doctor was unable to account for my symptoms or treat them effectively, and I was hopeful of getting better insight from a research scientist who I presumed would know more than a suburban general practitioner. I was furious about the diagnosis of hypochondria because that meant that even research scientists were useless to me i.e. they did not take my problems seriously and were doing nothing other than providing a worthless and insulting diagnosis, and had no intentions of trying to find a cure).In the process I had the opportunity to discuss my own results with a research cardiologist (fitness readings from zero to 350 and plateauing) and I asked him if that was convincing scientific evidence of my condition being real and physical. The exact words in his blunt reply were astonishing and given in a resentful tone of voice; he said “No! that means nothing!!!” I got the impression that he was jealous of a non-doctor making a credible scientific discovery and proving some old theories wrong, but I wasn’t trying to prove anything. My objective was to solve my own problems, and offending doctors was just creating more problems.Also I must say that I had courteous relations with most of the staff and doctors who were co-operating with me in the research, and because of my role as co-ordinator, I had access to the premises on a regular basis. However when I wanted to access my own file out of curiosity about the medical opinion given about me, I was advised that it was not standard practice to give non-doctors permission to read them. Nevertheless, I made a point of waiting until the staff were out, and went into the file room and read my own records. Within the text were the typed words “This man is a hopeless hypochondriac”. This made me furious so I stormed out of the building telling everyone in sight that they were all useless idiots. After calming down I apologised for my outburst, as most of them were not responsible for the remarks. In the meantime I decided that I could only rely on myself if I wanted to get any useful understanding of the problem.(Regarding the doctor who diagnosed “hopeless hypochondriac” – When I first met him I was suffering from dozens of symptoms, including breathing difficulties, faintness, and dizziness, and my heart was pounding violently in response to the slightest exertion. I vaguely recall having difficulty walking from my car to the Institute building, and then I found it difficult to get up the stairs to the medical room on the first floor, and then the slight effort of riding the ergometric cycle produced a fitness reading of zero. I was also withdrawing from a high dose of barbiturates, and decided to study medicine myself because my doctor was unable to account for my symptoms or treat them effectively, and I was hopeful of getting better insight from a research scientist who I presumed would know more than a suburban general practitioner. I was furious about the diagnosis of hypochondria because that meant that even research scientists were useless to me i.e. they did not take my problems seriously and were doing nothing other than providing a worthless and insulting diagnosis, and had no intentions of trying to find a cure).
| What I did to diagnose the problem | In 1975, after 3 years of health problems that were becoming relentlessly worse my symptoms became intolerable but my doctor was unable to diagnose my condition (because “there was no evidence of organic disease”) so I decided to start reading a few medical books to see what I could find. I soon found that my symptoms were consistent with Da Costa’s Syndrome (first identified by J.M. DaCosta in 1871)which is nowadays called The Chronic Fatigue Syndrome. |
| Why I attempted to treat the condition with exercise | Many of my symptoms were aggravated by the slightest exertion, and my general assumption was that my problems involved a deterioration in my physical condition, so I decided to treat the problem with some regular exercise under medical supervision. I made some enquiries and found that such a service was provided by the South Australian Institute for Fitness Research and Training so I enrolled in one of their courses. My immedicate objective was to use exercise safely to improve my level of fitness to a good standard and regain my health. After having my fitness assessed I designed my own fitness programme and proceeded to follow it while training within a large group of fitter, faster individuals. (I had to ignore the pressure to conform to the higher levels of training, which was partly due to the problem of persisting with training while I was always running last, and partly due to the negative remarks of some other runners). |
| My fitness level was scientifically measured as zero | In the process of training I also found articles in medical research journals which presented the general opinion that the condition involved a fear of exercise in people who had been protected from the vigors of sport as children (I had to give up my role as gymnastics instructor because of my health problems, so the idea that the symptoms were due to a fear of exercise was obviously wrong). I was provided with my own medical reports which showed that when I started training my fitness level was zero, compared with a normal healthy level of 900 and an athletes level of 1200. I was also told that the scores were determined scientifically using graphs of ergometric load over pulse rate so that the results were impossible to fake. (In contrast to my aerobic fitness level of zero, one of the staff told me that my subcutanious fat level was that of an athlete. This was measured by applying a caliper to the skin fold of my abdomen, and I can recall that the teeth of the calipers were virtually compressing two pieces of skin together with no fat between). |
| How I determined that my condition was chronic | I continued to train for 3 months and my level rose to 350 so I was becoming quite enthusiastic about the prospect returning to full health. I therefore trained more frequently for a further 3 months but at the end of that time my fitness level was still 350 so I had to consider three things. That my condition was measurable, and that it was abnormally low and not related to a lack of exercise, and that it was chronic and was not continuing to improve to normal levels despite regular, more frequent, and increasing levels of exercise. |
| Why I stopped training | I continued to train for a further 3 months when I damaged a knee cartilage and had to stop. |
| The first effective exercise programme for CFS | I was therefore the first person in medical history to design an exercise programme which was achievable for patients with chronic fatigue, and was the first to provide scientific evidence that it was a real, physical, and measurable condition. |
| I wrote a theory about posture and cfs | Four years later I wrote a theory which explained how poor posture could cause that type of chronic fatigue (there are many causes and types) |
| I co-ordinated a research programme on exercise and cfs and why all previous medical programmes failed | In 1975 I was invited to coordinate a research programme for other people with chronic fatigue at the Fitness Institute, and became the first individual to succeed in having such patients continue to participate in programmes (previous programmes which were conducted by doctors who thought that the ailment was due to a fear of exercise, all ignored the reality of the symptoms, and all failed. That was because the patients who followed the doctors instructions and tried to run at a normal pace would have developed distressing symptoms and lost confidence in the advice immediately. Most of the other patients refused to follow instructions or dropped out within the first few weeks – It was reported in the journals that “they could not, or would not train”.) |
| Bureaucratic requirements for research | In order to start the programme I had to get a small government grant and fulfill a few bureaucratic requirements. I wanted to establish that the condition was measurable so that other researchers would start trying to cure it (instead of ignoring it). I was advised to ask for a grant aimed at curing the problem with an exercise programme rather than measuring it’s severity. (this was because measuring the condition would give proof of disease and would require doctors and governments to take responsibility for it, but curing it would solve the patients problems and remove the governments exposure to the expense of paying for “another real illness”. |
| I found that many cfs patients had measurable and abnormally low aerobic capacity | While conducting the programme I found that some of the other patients with persistent fatigue had abnormally low scores which were not improving in the normal manner, as would be expected from healthy people |
| The value of scientific evidence??? | |
| 80 patients with cfs were medically assessed | I continued the research programme for about 2 years but eventually had to stop for health reasons. During that time more than 80 people with chronic fatigue were medically assessed and commenced training. Several of them continued training for 2 hours, twice per week, for 3 training periods of 3 months each – more than 9 months, and were still training when I left the programme. One of them participated in a 6 mile marathon. I have maintained reasonable health for myself since then by walking 10 – 20 kilometers per week at a casual pace. |
| What I did about bureaucratic obstacles | About 5 years later I was able to find another medical opinion about my own health by going through the difficult task of weaving through bureaucratic obstacles associated with The Freedom of Information Act, and I found information which was supposed to be hidden from patients, and the typed words were “this man is not ill, he only believes he is”. “He is the leader of a self-help group and acknowledging his condition would have a bad influence on the others”. (I tried to solve some my health problems by establishing several self help groups for patients with chronic fatigue, and chronic abdominal pain, essentially because doctors were not providing any effective treatments). Most of the statements in the report were misrepresentations of what I said, and some were the exact opposite, with the obvious intention of discrediting my opinion. When I discussed my symptoms with him before he prepared the report I described fatigue in relation to exertion, and abdominal pain in relation to repetitive bending at the midriff, and he tried to create the impression that I was an ignorant person who didn’t know his own mind and gave the diagnosis of anxiety hysteria (that I was converting psychological problems into imaginary physical symptoms, or that I had an exaggerated fear of trivial disease). He wrote “There is nothing at all to find on complete general examination.” |
| I obtained evidence of biochemical abnormalities in cfs from Newcastle University | About another 5 years passed when I heard about some researchers in Newcastle University (of New South Wales) who had found evidence of metabolic abnormalities in chronic fatigue by examining the chemical profile of urine, so I sent a sample of my urine to them with the appropriate fee. They returned two results consistent with the most severe level of chronic fatigue. |
| CFS was officially recognised as a medical condition by the AMA | The Australian Medical Association accepted that chronic fatigue was an officially recognised medical condition about 10 years later (in the 1990’s). |
| Modern exercise programmes for cfs | Nowadays there are many exercise programmes on offer as treatments. All modern exercise programmes use similar principles to those that I used in 1975 and 1980 when I established that it was possible for most people to gain a moderate improvement in health, and in a small number of cases a return to normal levels of fitness. They involve starting with very mild exercise (walking)) and progressing slowly. |
| Current medical attitudes | However, I still see articles which repeatedly refer to the problem as an anxiety disorder for which there is no organic evidence, which is not measurable, and simply involves a fear of exercise, or is just tiredness. M.B. |
The History of Science and Serendipity
It has been a common enough observation from scientific history, that the answer to a mystery will be staring thousands of people in the face, before someone who is looking for it, sees it, and recognises it’s value.
I therefore presume that in 1976, when I saw that my own fitness reading was scientifically measured as zero, that I was the first person to recognise it as evidence of a measurable physical cause of a health problem, because I was looking for it, and nobody else was.
I can only suppose that thousands of doctors had seen that data before me, mixed in with data from other types of patient in fitness programmes, and have routinely assumed that it was due to lack of exercise resulting from laziness, or due to a fear of exercise.
It should also be staring any reasonable person in the face to note that, if I was afraid of exercise I would not have tried to treat my health problems by deciding, entirely on the basis of my own considerations, to volunteer for a fitness training programme, and I would not have continued with it for the best part of a year, ultimately for 2 hours per day for 6 days of the week. It is also stating the glaringly obvious, that if I was a lazy person, I would not have started reading medical books in order to solve a problem which was, as I was led to believe, beyond the comprehension of my doctors, or anyone else in the medical profession for the previous 3000 years. (I didn’t think that it would be an easy thing to do, and the study involved sitting at a desk, which was causing me a considerable amount of pain, but the task was, without any doubt of mine, an absolute necessity – This was because I had been following medical advice and taking the prescribed medications for several years, yet my health continued to deteriorate, and there was no evidence that anything was going to alter that course unless I did something about it myself).
Unfortunately there is a strategy called spin, which enables data and evidence to be dismissed, trivialised or ignored entirely, and will only ever be found by those who look for it.
When Galileo found evidence that the sun was the centre of the universe rather than the earth, his book was confiscated and he was put under house arrest, because his ideas contradicted those of the church. The church authorities new of the truth, but did everything they could to stop the public from finding it, or believing it.
Semmelweis discovered that women were dying of child bed fever because surgeons were using the same instruments that had been used and contaminated in autopsy studies. However this offended other surgeons who blocked his promotion to the position of clinical professor. They also refused to cooperate with his methods of disinfecting their hands and instruments with chloride of lime, and as a result, many women continued to die unnecessarily. Such frustrations eventually sent Semmelweis mad, presumably because he didn’t know enough about history. M.B
A Useful link on the politics of CFS
One of the objectives of my exercise research programme was to scientifically prove that chronic fatigue was due to a real measurable ailment and that it was not just imaginary, and not just normal tiredness, and the programme was entirely successful. A second objective was to determine if continued participation in that programme was effective in relieving symptoms and improving stamina, or curing the problem. The results clearly indicated that most of the individuals who participated did improve their fitness, but reached a level that was still below normal, and stayed that way regardless of continuing to exercise, and only one appeared to have returned to normal levels.
In other words the success of that programme scientifically proved that people who were persistently troubled by fatigue had a real physical condition, and that it responded favorably to three to nine months of training, and that it was, in most cases, not a cure. It was useful to some patients but only those who wanted to try it, and, obviously no person should be forced to do it, or to increase at a rate that aggravated their symptoms. The fact that they reached a degree of fitness that would not continue to improve even if they exercised also proved that they were not lazy, and that the fatigue was chronic.
I had also read the psychiatric literature and found an idea that might be useful called Cognitive Behavioural Therapy, which simply means ‘changing the information that a person has to relieve a problem’. In particular, if a person has chest pain and think it is due to their hearts, and a doctor tells them that they don’t, they won’t believe it, and will worry. However if you change the information that they have, by explaining that the chest pain is in muscles to the left of the chest, and the heart is in the centre of the chest, they may stop worrying unnecessarily about their hearts. The problem is, of course, a bit more complicated than that, but the general principle is appropriate.
I did my research in the early 1980’s and since then the term ‘chronic fatigue syndrome’ has become popular, and many research programmes have been conducted under the name of GET or PACING which means, in plain English – Graduated Exercise Training, or, walking or running at a pace that is that is within your own limits i.e. exercising within your own personal limits – and by extension – keeping within your own limits in terms of general lifestyle. Also Cognitive Behavioural Therapy has been abbreviated to CBT, and both methods have become the most popular forms of treatment.
However, some people have been deliberately trying to misrepresent those ideas, and the disinformation has become so effective that those methods have been disputed by people who actually study CFS, or run CFS societies, or actually have CFS.
The types of disinformation include . . .
The false claim that GET is a useless treatment because it doesn’t cure the problem.
Here is the facts . . . ‘You can’t cure every case of CFS, but it is still a useful method for improving the stamina for some patients, and it is still a useful reproducible method for scientifically proving that it is a real physical illness.
The following quotes come from a website that has some very useful information about the politics of CFS, but I was reluctant to use it because it is critical of Graduated Exercise Training, and Cognitive Behavioural Therapy.
“There can be no doubt that, for patients with ME/CFS as distinct from those suffering from chronic “fatigue”, neither CBT nor GET is effective, otherwise everyone would by now be cured . . . The apparent intention of the PACE Trial Principal Investigators to remove people with ME/CFS from receipt of state and insurance benefits raises a larger question than just welfare reform. It is also about the way illness is being redefined and reclassified and about why this is happening and about what forces are at work in this process of redefinition”.
See here http://www.meactionuk.org.uk/Can-the-MRC-PACE-Trial-be-justified.htm
My main point here is to say that people with CFS need all of the scientific evidence that they can find, and shouldn’t be dismissing good studies, and should look toward a co-operative approach to other people who are trying to solve the same, or similar problems.
The people who want to discredit the reality of CFS are deliberately spreading disinformation to create confusion, and they want nothing better than to have CFS groups arguing with each other.
***
While I was contributing to the Da Costa’s syndrome topic in Wikipedia I had two critics named WhatamIdoing and Gordonofcartoon who were essentially doing as much as they could to delete the information and ban me and steal the information, but also misrepresent it and spread disinformation about the symptom of chronic fatigue. Their choice of wording on many topic pages before and since has been aimed at confusing normal fatigue with chronic fatigue to create the impression that they are the same. One of them has won a “prize” for writing an essay on ordinary fatigue caused by work, and is obviously raging with jealousy about me, because I have done real research, in a real research institute about a serious disabling condition of chronic fatigue.
That individual has recently written an article called “Cancer-related fatigue” which includes this statement at 1:33 on 7-10-10
“Cancer-related fatigue is a chronic fatigue (persistent fatigue not relieved by rest), but it is not related to chronic fatigue syndrome.[2] See here http://en.wikipedia.org/w/index.php?title=Cancer-related_fatigue&diff=prev&oldid=389218805
Since then that editor has found a reference for that, but I have actually had the chronic fatigue syndrome for 35 years from 1975 to 1010, and cancer and chemotherapy for 8 years from 1994 to 2000, so I actually know the difference, and yet that contemptible fool has made snide remarks about ‘anecdotal evidence’ being ‘unreliable’.
Most other editors will never notice that the ‘Cancer-related fatigue’ page was started by the same individual who is linking many other topic pages back to it.
That self-proclaimed ‘instant expert’, who has the impressive memory of a parrot, but only the brain power of a flea, and the ethical standards of a fork-tongued rattlesnake, has stolen that general information from me.
Nobody could say with any authority that they were different unless they actually had both illnesses, because there is no “officialy” “acceptable” scientific way of measuring either of them. I have said that the chronic fatigue syndrome was not made any worse or any better by the 8 years of ‘non-Hodgkin’s lymphoma, or by the two years of side effects of chemotherapy, and that a different type of fatigue only occurred occasionally for short periods of time about 2 weeks after each of five sessions of the CHOP type of chemo. The temporary nature of that fatigue made it trivial compared to the chronic fatigue syndrome. Since recovering from the chemo side effects the chronic fatigue syndrome is no better or worse than it was before I had the chemo. For more information see here https://theposturetheory.twebexponent.co.uk/about-the-author/#anchor260609
People with the chronic fatigue syndrome are attempting, under difficult circumstances, to do the right thing by finding scientific proof to confirm the reality of the problem, and that editor is doing everything to hide and discredit it, so CFS patients should do everything they can to get rid of the toxic influence of that individual who is an insidious pest.
An organisation, such as an insurance corporation, is either paying them to confuse the issue of chronic fatigue, or that editor is ingratiating themselves by doing the type of dirty work that will get them some sort of social or financial gain in the future.
Essentially, insurance companies are making profits by claiming that if you make weekly payments into their funds, they will make payouts to individuals if they later develop ‘medically diagnosabel’ illnesses‘ called MDI’s, but what they don’t tell you is that only 50% of illnesses are “medically diagnosable” to the extent of “official recognition”, so 50% of people who pay premiums and become chronically ill, don’t get payouts. i.e. the insurance companies make profits from 100% of premiums, but only honor 50% of their contracts.
There are now clear warnings on cigarette packets which say ‘Smoking causes lung cancer’, and there should be consumer warning’s on the front page of insurance or superannuation contracts . . . ‘Only 50% who become become chronically ill will get payouts’. The percentage might not be accurate, but the concept of the problem is.
Another problem that you will need to deal with if you develop CFS is that you may find yourself in a court room where the burden of proof will be foisted onto you , and your opponents will be a highly paid team of scientists, doctors, psychiatrists and lawyers. Such imbalances need to be corrected.
I tried to stop 200 million chronic fatigue patients from being swindled out of their entitlements the way I was
In 1975 I was extremely ill, but nothing showed on blood tests or x-rays so I was told that there was nothing physically wrong with me and sent to a psychiatrist who asked various questions which had absolutely nothing to do with my symptoms so it was obvious to me that he wasn’t interested in discussing a physical cause.
My health problems were almost exclusively aggravated by my work as a clerk so I continued to get worse and had to ultimately leave work, and in that process I applied for superannuation benefits which were about 40% of my salary, which was much higher than a standard pension. However, I didn’t want to be branded as a retired public servant with a mental illness because that would make it difficult for me to get a job in the future, if I ever recovered.
I also didn’t want to go through a process where a tribunal of men twice my age would badger me with questions and demand proof of disability when I didn’t have any medical evidence to back me up, so when I was told to go back to work and work hard or be sacked, I went home home and wrote a letter of resignation the next day.
My health problems were extreme, and I decided that it was better to leave my job alive and sane rather than being harassed and made worse.
In other words I was effectively swindled out of my entitlements.
The only sensible thing to do was to study medicine very slowly myself, and try to determine what was wrong, and develop my own ways of treating it, but despite all the success I had in that regard, it took me more than a decade to feel as if I was barely normal, but my health was still unstable, and not until more than 20 years was it reliable, but then, it was only reliable and stable if I stayed within my limited capacity for exercise, work, and life in general. whenever I exceeded those limits, which I frequently tested, I would have problems again, ranging from short term and mild, to months of unrelenting pain or fatigue.
During that time i discovered that my ailment is very common, affecting 2-5% of the population or 200 million people world wide and that the cost of paying insurance, pensions, or compensation for a lifetime is something that large organisations would not like to pay.
I have also learned that the motive of many of the people in those industries is to maximise profit and minimise costs by any legal, or illegal method that they can get away with.
I therefore decided to help the other 200 millions patient avoid being swindled out of their entitlements by searching for and finding the information they needed to succeed.
For example, there is scientific and medical proof that the condition can be reliably diagnosed, but some people are being paid to hide it form the patients, or delete it when it becomes available (e.g. see here), or it is not being “officially” accepted, and there is proof that it is chronic, but the organisations pretend it only lasts for 6 months and is likely to return to normal.
The organisations also know that the patients are often able to lead basic lives, but if they try to lead a normal life they will soon become crippled with pain or fatigue, but rather than discuss or consider that, they pay photographers to take photos of the person and use it as false evidence that the person should be able to work in the normal way.
In the process I have seen many patients get injured or ill, and claimed that it is their “right” to get compensation and other benefits and have been paid large sums of money, and now live in large houses, and drive in modern cars, without knowing that I made it possible, while I am living in poverty, and being treated like a bludger a fool, and a loser.
I have taken enormous risks with my health, in experiments to learn how to manage the problems when no-one else could, and I have never been bothered by people taking photos which might be used in court to prove I am healthy, because if I stayed home behind four walls I would be described as a mentally ill person who was afraid of the world, or I would actually go nuts from social isolation.
From an insurance perspective, people who go mad, commit suicide, or die, don’t cost them anything, whereas those who are alive and sane can.
The advantage I have is that I now understand and know how to manage my health so that the only problem is my limitations, and if I had my life to live over again, I would be able to use those methods from the start, to be much more successful in money making activities instead of having to spend much of my time studying my heath, and leaning how to control the symptoms.
The disadvantage is that representatives of the type of organisations who swindled me would still be defaming my character, and at the same time stealing my ideas so that they can claim the credit, and use them to minimise their costs, and there are 200 million patients who have benefited from my research and methods, and don’t know that I exist, or that I am the reason the are able to gain their benefits.
I was hoping that eventually, the millions of patients who I helped would support me, and thank me, given that I was only one person at the start with all the odds against me, but some of them treat me like dirt.
See also here.
The video below describes the five main 5 reasons which are used to deny patients their legal disability entitlements, and are typical of the methods which were used to swindle me thirty nine years ago, and will continue to be used against patients who wait for others to help them, instead of studying medicine and doing their own fact finding. It was provided by Tom Kindlon on Twitter 27-9-13.
Note how insurance companies pay highly qualified doctors to swindle genuinely ill patients who have never read a medical book in their lives. They have no more hope than lambs to the slaughter.
See also how the pain of sitting at a desk was real, and physical, and I was told it wasn’t, and how I eventually reduced it to a minimum by developing the stand up computer posture here. Note that I can now sit at a desk in some situations but it is my copyright which I will protect by not describing it.
Long term follow up studies
While a small number of people with the chronic fatigue syndrome may recover, and others may appear to, the fact remains that it is generally a chronic condition.
Relapses are a common feature, especially in the first few years, until the person identifies the factors which determine the symptoms and uses that information to prevent them. However, even then, they still have their physical limitations, and can only control their symptoms by staying within them.
A former name for the condition was Neurocirculatory asthenia, and a good follow up study is . . .
Wheeler E.O. (1950), Neurocirculatory Asthenia et.al. – A Twenty Year Follow-Up Study of One Hundred and Seventy-Three Patients, Journal of the American Medical Association, 25th March 1950, p.870-889 (Contributors to the study: Edwin O.Wheeler, M.D., Paul Dudley White, M.D., Eleanor W.Reed, and Mandel E.Cohen, M.D.)
A more modern study is by By Molly M Brown, David S Bell, et al. June 30, 2012 Understanding Long-Term Outcomes of Chronic Fatigue Syndrome – Journal of Clinical Psychology, June 29, 2012. See ProHealth.com • June 30, 2012 here
The following quotes come from it . . .
“Study suggests many patients once labeled ‘recovered’ from CFS are merely less disabled, underscoring the need for effective treatments, and for studies applying newly implicated biological markers / diagnostic criteria.” . . . and . . . “it appears that individuals who maintain a diagnosis of CFS for more than two decadese continue to report a high level of disability, as participants in this study scored at least one standard deviation below general population means across all MOS SF-36 subscales except for Mental Health (Jenkinson, Coulter, & Wright, 1993). Perhaps the most important findings in this study pertain to the remit group, which accounted for 80% of the 25 CFS participants. Given the duration of the follow-up, it would be expected that the remit group would demonstrate comparable functioning to a group of healthy individuals.
Yet this group had significantly more impairment than controls on 21 of the 23 outcomes evaluated” (end of quote).
The consequence of not paying pensions and other benefits
It is very clear that most people who have chronic fatigue syndrome will have it for life, and that insurance companies and governments don’t want to pay those costs, so they would prefer the suggestions of researchers such as Simon Wessely which they can use as a plausible excuse for denying entitlements. The following words are a quote from another website about his ideas . . .
“Simon Wessely was showing up at actual
DLAAB meetings as far back as 1993 being noted as giving messages
like- “As regards benefits:- it is important to avoid anything that
suggests that disability is permanent, progressive or unchanging.
Benefits can often make patients worse.” . . .
Is it any wonder therefore
why it’s so hard for ME/CFS patients to obtain disability coverage, or
why the UK Govt. is oh so fond of ‘Dr.’ Wessely?” (end of quote) See here and here.
The fact remains that patients with CFS will actually be much worse off if they are not given benefits, because the addition of “poverty” to their situation is definitely not going to help anyone except those organisations who don’t have to pay the costs.
One of the consequences of being denied benefits is undoubtedly depression, with some studies reporting that 50% of patients with chronic fatigue become depressed after five years. See my report here
Two editors try to hide the long term aspects of Chronic fatigue from the readers of Wikipedia
See how 2 Wikipedia editors try to hide the long term consequences of chronic fatigue syndrome by deleting a 20 follow up study by Edmund Wheeler in 1950 here.
“Certainly, there is no test — a fact that insurance companies in the past have used to their advantage. Even now many insurers won’t cover ME.”
Another quote from an interview with Simon Wessely about the chronic fatigue syndrome published in The Times 6th August 2011 . . .
“Theirs is a debilitating physical disease for which, some insist, there is, as yet, no cure. Certainly, there is no test — a fact that insurance companies in the past have used to their advantage. Even now many insurers won’t cover ME. Should they? “Obviously I’m of the view that we should treat these disorders equally, which is, I think, getting rid of the distinction between neurology and psychiatry.” He said this wouldpartly get rid of the distinction between the “deserving” and “undeserving” ill. See here.
See also how insurance companies maximise their profits here.
and how an anonymous Wikipedia editor creates prejudice against patients here.
See another report on the economics of this topic here.
The breathing abnormality in Da Costa’s syndrome and CFS ©
Based on my book called The Posture Theory and first published on this website on 4-6-11
There is a characteristic type of breathing in CFS that is so typical that it’s observation has been used as a means of diagnosing the ailment.
If you watch the person for awhile you will see them occasionally take a more forceful and deeper breath that ends with a sudden stop and be followed with normal breathing. There is sometimes the sound of air rushing into their mouth and a heave of their chest as they do so.
The patient will say that they felt as if they needed extra air, and that they couldn’t get as much as they wanted because it felt as if they had met some type of obstruction.
To understand that symptom it is necessary to know how normal breathing occurs. Essentially the body has two major cavities or spaces. The upper one is called the chest which contains the heart in the middle, and the lungs on each side. The lower cavity contains the stomach and liver etc.
The two spaces are separated by a large broad muscle which includes several holes such as the one which allows the food pipe to pass through to the stomach below. It is called the thoracic diaphragm and is dome shaped, and as it contracts the central part descends and drags the lungs downwards and creates a bigger space in the chest, and hence a vacuum which draws air in through the nose and down the throat to the lungs. The lungs are elastic like rubber bands, and are attached to that muscle, so when they are dragged down they are stretched. Therefore, when the muscle relaxes the lungs draw it up again. As it rises it pushes air out of the lungs, up through the throat, and out through the nose.
Hence breathing occurs because the contraction and expansion of that muscle draws air in and pushes air out of the lungs.
When the person with CFS feels as if they haven’t got enough air, they try to contract that muscle as tightly as possible. but it can only draw in a small amount extra, and won’t contract any further, which is why they sometimes feel as if they are “breathing in as if against an obstruction“, and why they say that they feel as if “they can’t get enough air”.
That individual may breath normally for an hour or two and then take such a breath, and continue to breath normally but take such breaths periodically throughout the day. The frequency depends on how much energy has been expended and how much oxygen is required to cover the requirements of such things as sitting, standing, or walking etc.
Healthy people have biological monitoring mechanisms which ensure that as the level of exercise increases the level of oxygen use increases to cover the energy needs precisely. However, in CFS, the breathing process is inefficient, and at rest there is not much difference to normal, so the symptoms only occur occasionally. Nevertheless, during exercise the abnormalities and inefficiency of breathing increases out of proportion as the level of exertion increases.
In practice that is evident by the fact that, at rest, the person may take occasional forced and deeper breaths, and when walking they may take such breaths more often. When the level of exertion is increased by jogging the person may actually have to stop after fifty yards and take two or three forced deep breaths, and then continue. Generally speaking, based on my experience, if I haven’t gained enough extra air in that process I will continue anyway and sometimes stop again in another ten yards and take another forced breath. and then proceed for another 50 yards. When jogging for a mile I may have to stop many times, usually taking from one to three breaths before continuing, and occasionally have to walk for fifty yards, and then stop, take some deep breaths, and continue jogging again.
Exercise at higher levels may in some cases be impossible because the difference between the energy being expended and the oxygen being usefully supplied is too great, and it can result in more significant gasping which is unpleasant and draining and takes excessive amounts of time to recover from.
That is why most patients will refuse to participate in exercise programs where they are required to keep on increasing their levels of exertion every week. Sooner or later they will reach their limit, and leave the course.
At rest the feature is just a forced breath, but sometimes I will need to place my hands on my hips to gain extra leverage and force the breath deeper. However. when I am jogging I will generally stop, and then bend at the hips and put my hands on my knees, straighten my back, and get even more leverage to gain the maximum depth of breath possible. It seems to be more effective in supplying the extra air I need.
The frequency of the extra breaths may also increase while talking if the amount of air exhaled in producing voice sounds is reducing the air available to the lungs.
That breathing abnormality is different to normal sighing or yawning, and different to asthma, and is different to the general concepts of hyperventilation where the person will be described as panicking and then breathing rapidly for several minutes until they become dizzy. It is not due to lack of exercise.
The CFS anomaly can and does happen any time of the day or night when the person is resting comfortably or when they are watching TV comedies, dramas, or sports. The only factor which seems to influence the symptom in my experience is the level of exercise.
To view some 3D video’s on the normal breathing process see here and here
For my YouTube video on this topic see here http://www.youtube.com/watch?v=iGts2nfGtY0
The benefit of experience
My original reseach concepts were copied by London researcher Simon Wessely from my 1982 study, and I added the essay below, probably in response to criticism from 2 Wikipedia editors, in about 2008, and it has been copied by Simon Wessely’s colleague Peter White who set up a five year study of CFS and exercise a few months later.
If you read the medical literature about patients with chronic fatigue you will get the general impression that the difficulties they have with exercise as adults are the result of not having any experience with normal exericise during childhood. The following words are extracted from a 1956 book . . . ” At school kindly doctors and soft mothers protected them from the hazards of football, swimming and the gymnasium . . . and . . . Fear of football, and fear of swimming are common in childhood.” (end of quote).
However, I played a lot of sport when I was young and was a good swimmer and a gymnastics instructor, so when I developed the chronic fatigue syndrome and read that opinion I was able to see that it was ‘plausible but not factual’. I was also able to notice and describe the differences in the response to exercise, and was invited to design and co-ordonated a research program to scientifically measure and evaluate those differences.
One of the features of good health is often described by marathon runners who will say that they were able to run the first few miles with relative ease, but would become fatigued later in the race. They typically ignored that fatigue and persevered until they got their ‘second wind’ and could continue to finish the race without any further problems.
That aspect of exercise is common knowledge and well known to runners, or anyone who has played a lot of sport, so it tends to be taken for granted as a characteristic of all types of fatigue.
However, with chronic fatigue that ‘second wind‘ generally doesn’t come, and in fact, persevering despite the fatigue can make the problem much worse. The fatigue tends to continue getting worse until the person can’t keep going any more, and then, instead of recovering within a few minutes, it may take days or weeks.
Consequently if the person does actually have an exercise related fatigue problem then it is not appropriate to give them a ‘graded’ set of exercises to do where they have to increase the level each week, every week, until they recover to normal health, because as soon as they reach their limit they will start having more problems than benefits, and will almost certainly refuse to continue.
To conclude, I can say that telling a person who is healthy to ignore their fatigue, think positively, and get through the fatigue barrier may be an appropriate and effective way of getting them to improve their fitness. However, giving that advice to someone with exercise related chronic fatigue is the worst thing that you can do, which is evident from the reports from 100 years of graded exercise programs. It is also not sensible to argue that other patients with fatigue regained their fitness, therefore eveyone should be able to, and it is not aceptable to ‘blame the victim’ for the failure of the inappropriate program design.
The individual needs to recognise that their physiological response to exercise, fatigue and perseverance is different, and they need to learn their limits and stay within them. The reduced levels of exercise can still improve the tone of the cardiovascular system and their physical fitness to whatever level is practical and possible.
It is apparent from the different responses, that each individual needs to be assessed before they start training to determine what type of fatigue they have, and what type of programme is most appropriate to their requirements.
See the programme that I designed in 1982 here
An article by Andrew R Lloyd in the Medical Journal of Australia in 2004; 180 (9) p.437-438 (which confirms the effectiveness of a fitness programme which has exactly the same principles as the program that I designed 22 years earlier) here
Some newspaper reports on the controversies about CFS exercise programs in 2011 here
The copycats who have stolen my ideas
(without having my knowledge and experience)
This section was written on 6-10-13, and is a comment on why the researchers who copied me have caused so many problems for patients
I developed my ideas and methods of treating chronic fatigue with exercise based on my personal experience and research for seven years from 1975 onwards. After a brief discussion with the head of a research institute it was obvious to him that I could solve an international research problem, so asked me to design an exercise program in 1982. He also asked me because his other researchers were busy, and he knew that I could organise such a project. Everything went according to plan precisely, but if there were any problems I could understand them, and give advice about what to do immediately.
However, since then I have suspected, and confirmed that some researchers have been stealing my ideas and copying me, and giving the false impression that it was their “new” method, I didn’t know anything with any certainty, but in December 2012 I read that a London psychiatrist called Simon Wessely had been given a prize, and soon after that a knighthood for his contributions to that area of study, and then his colleague Peter White finished a study of 650 people with chronic fatigue about an exercise program called the PACE trial.
It is virtually a copy of my methods, and yet follow up studies have found that 51% of patients have been made worse, rather than better.
The difference between copycats such as Wessely, and me, is that when patients report problems, Wessely doesn’t know why, and he doesn’t know what to do. The best thing he can do is “guess” and make mistakes at the expense of the patients health, whereas I know what the problems are, and know what to do.
They also don’t have the benefit of my 28 years of additional experience with the short term, and long term, positive and negative effects of all types of exercise under a wide variety of circumstances.
Education and Cognitive Behaviour Therapy
From pills and psychotherapy in 1975, to GET, Pacing, and CBT in 2013
Word meanings
Cognitive – related to the thinking process of the brain
Behaviour – how, what, and why a person thinks something
Therapy – treatment
The word cognitive behaviour therapy refers to process of telling a person something which will change the way they think about something in order to change or improve it. For example to stop them from worrying unnecessarily.
When I was young I had occasionally chest pains, and although it didn’t worry me, I wanted to know the cause for the common sense purpose of ensuring it wasn’t the sort of problem that needed to be treated before it caused a problem.
Therefore I would ask a doctor what was causing it. However, some doctors assumed that I was worried, when often I was just asking a question, and instead of telling what was causing the pain he would say “it is not your heart”.
Consequently I was curious to know the cause when I began studying my own health problems in 1975. I eventually came to the conclusion that it was due to my slightly stooped spine which was causing me to lean forward and put the repeated pressure on my ribs and cause inflammation and tenderness in the tissue between them which would occasionally result in a brief and sudden sharp twinging pain which would dart from the front of my chest on the left side, toward my back for about 2 or 3 cm.
I also found a book by Britain’s top researcher in the 1950’s who came to a similar conclusion, that faulty posture, or bending at an awkward angle might be the cause, and he gave the example of bending to crank a car engine.
However, he also considered that emotional factors such as anxiety might be altering the breathing of the patient, where the constant strain on the breathing muscles, which were attached to the chest wall, might be the cause.
Despite him considering both possibilities the postural cause was forgotten, and the majority of people believed that anxiety was the cause, which is probably because my doctors never told me anything about it.
When I was invited to design an exercise program for chronic fatigue patients in 1982, I also included methods of relieving any concerns that the patients might have about the pain being caused by heart disease, so I recommended that they be given a brief talk in the introduction, about the various differences between they symptoms of chronic fatigue, and those of heart disease.
For example, I recommended that patients be told what the cause of the chest pain was, not what it wasn’t.
I knew that my ideas of physical cause were not popular with some psychologists so I decided to appease any opposition they might have, so instead of discussing that as a common sense way of providing useful information, I called it “Cognitive Behaviour Therapy“.
Thirty years have gone by since then, and in the past few years I have noticed that many other people have been copying my methods, but instead of giving me the credit, they have been claiming, or being given the credit, which is ‘stealing’ my ideas.
The main treatments which existed in 1975 were ‘medication’ and ‘psychotherapy’ where the patient would be asked about worries, personal matters, and traumas of childhood etc.
The methods which I developed now dominate all modern discussions and treatment methods, and include . . .
Graded Exercise Therapy – which refers to treating the fatigue by improving fitness levels, by starting at very low levels, and gradually increasing, but within each individuals limits. (many people are not copying that method properly)
Pacing – which refers to doing things such as exercise, or the general activities in life at a rate which doesn’t wear the person out, and explaining how to do that.
Cognitive Behaviour Therapy – educating the person about the cause of their symptoms to appease any concerns they may have had about their hearts, or other health problems, and how to efficiently tone down any stress, emotions or other factors which may be having an influence on their symptoms.
You can see how I referred to such things in the guidelines I wrote for the instructor in 1982 here.
See also some of my reports about the chest pains here and here and here.
The Copy Cats
Before you read my report on the researchers who have copied me, stolen my ideas and methods, or become involved in the same research after me, see my research paper from 1982 here, and my experience with exercise before and after I developed chronic fatigue here. Many of their findings are the exact equivalent of scientific PEER REVIEWED CONFIRMATION OF MINE.
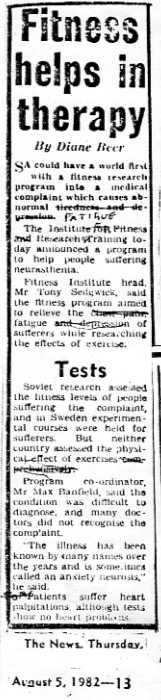
One of the news report, August 5th 1982
When I developed my methods of treating the symptoms I knew with certainty that they were not not just relieving them effectively, but were actually changing the situation form one in which they were getting worse to getting better, and I also knew that mine were far better than any methods from the past. I also knew that in the future other researchers would have to copy me or fail.
However, I couldn’t be certain that they would accept those ideas, or admit that they were mine. I just kept developing those methods, and refining them to deal with various health problems as it became necessary, and publishing how I did i to help with the general understanding of the ailment.
However, it has recently become obvious to me that literally thousands of top researchers have been copying me, or getting their ideas from those who have.
This is a quote from a research paper by Leonard A. Jason et al called “Non-pharmacologic Interventions for CFS – A Randomized Trial, published in the Journal of Clinical Psychology in Medical Settings, 14, 275-296. See here.
Before you read the quote I would like you to notice that they are not “medications invented by doctors’, and not ‘psychotherapy invented by psychologists’.
They are practical physical methods for treating a physical problem that were invented by me, and copied, reworded, or stolen from me and attributed to other authors.
The following quotes from that article are typical . . .
The purpose was to evaluate “nurse delivered non-pharmacological interventions . . . in the present study , 114 participants diagnoses with CFS were randomly assigned to four 6 month interventions“
“This treatment was featured in an influential review article (Whiting et al., 2001) . . . Using this approach, patients with CFS are encouraged to engage in gradual and consistent increases in activity and to attempt active strategies in place of activity avoidance as methods to manage symptoms (Surrawy, Hackmann, Hawton and Sharpe, 1995)”.
“Two randomized controlled trials of CBT (Deale, Chalder, Marks and Wessely, 1997; Sharpe et al., 1996) reported substantial improvements in physical and role functioning for the majority of treated participants with CFS”.
“Other non-pharmacological intervention studies have emphasized the role of aerobic exercise in the primary intervention. For example, Fulcher and White (1997) compared graded aerobic exercise to flexibility/relaxation training and found that patients with CFS in the exercise group were more likely to rate themselves as “improved” when compared to those in the in the flexibility/relaxation group (52% versus 27%)”.
“The CBT treatment was developed in Collaboration with Vincent Deary, who has worked for many years with the team a successful controlled clinical trial of CBT in CFS (Deale et al, 1997). This treatment was collaborative, educative, and negotiated with participants based on a comprehensive cognitive behavioural emphasis, Specifically, participants were asked to evaluate the effect of gradual and consistent increases in activity and utilize strategies other than avoidance. The aim was to show participants that activity levels could be increased steadily and safely without exacerbating symptoms.” (end of quote from page 280).
I have to emphasise that I am not accusing those researchers of stealing my ideas, but I can say with certainty, that I was the patient who invented those ideas in 1976 to treat my own ailment, and that I scientifically proved that other patients could benefit from the same methods in 1982.
Those researchers owe me a debt of gratitude for my ideas, and are doing a lot, such as providing a peer reviewed verification of my discoveries, but what they are definitely not doing is being the first.
They also need to acknowledge that the methods were developed by a patient, and not a doctor, and not a psychologist, and that the person was me.
I can also say with absolute certainty that after 38 years of practical experience that I know a lot more than those teams of experts, and that they are having some problems because they are doing things in slightly different ways.
Correcting “inappropriate illness beliefs”???
from “run faster and faster” to “exercise within limits”
Modern research papers about CFS refer to the process of correcting inappropriate “illness beliefs” as if it is just the patients problem, when in fact, when I began studying medicine in 1975, I found that doctors and psychiatrists had many mistaken beliefs about the nature of my illness, so I wrote essays to assist them to understand it better, and develop more effective methods of treating other patients.
For example, when ever patients asked what was causing their chest pains the doctor would say it was not their hearts, which would leave them in a state of doubt which can cause worry where it didn’t exist.
I found that the chest pain was caused by inflammation of the ribs on the lower left side, so I recommended that, in order to remove any anxiety they should “tell the patients what the cause is, not what it isn’t”, and some of them will stop worrying.
To put it another way I said ‘give them the facts to change their wrong beliefs about the cause of the pain.
For example the majority of doctors believed that the symptoms were mental and “not physical”, and were, “trivial” or “imaginary” of “all in the mind”, so they would tell the patients to ignore their symptoms and do whatever they wanted, and wouldn’t get any problems.
In particular, they told their patients that the symptoms they experienced during exercise were normal and that they should just ignore them and run faster and faster until they regained normal fitness and health.
Since I wrote my essays and books the treatment of CFS has changed entirely, and is now virtually the exact opposite than it was before.
Doctors are now educating their patients about their illness in a process called “Cognitive Behaviour Therapy” where their objective is to correct any inappropriate illness beliefs, and they are telling the patients they need to exercise within their limits, and improve gradually in a manner that doesn’t cause problems, and to slow down if it does.
Unfortunately for one reason or another, nobody wants to admit that I brought about those major changes.
In fact, Simon Wessely, a psychiatrist, has copied my ideas, and been given the credit, to create the illusions that psychiatrists brought about those changes. It saves them having to publicly admit to the embarassng fact that they were proven wrong by a patient. See more here, and here, and here, and here, and a section on my publications page near the end here..
See also my report on the somatororm diagnosis, which is offensive and ridiculous, and mostly victim blaming nonsense here.
Quotes about inappropriate illness beliefs in CFS
from a link provided by Tom Kindlon on Twitter 30-9-13 to criticisms from the editors of Phoenix rising website
See a modern report where the researchers still believe, and treat the chronic fatigue syndrome as if it is due to lack of exercise and inappropriated beliefs about illness and the effect exercise has on them here
This is some quotes from that article . . .
“I have a funny story about this clinic and recovery. I have heard that as part of the programme people who had previously been on the programme, who were now said to be recovered (by those running the programme), were brought in to meet with patients who were currently the programme. But after talking to them, the patients currently doing the programme realised that these “recovered” patients, were not in fact recovered at all!!
“Results: Poor outcome was predicted by membership of a self-help group, being in receipt of sickness benefit at the start of treatment, and dysphoria as measured by the Hospital Anxiety and Depression scale. Severity of symptoms and duration of illness were not predictors of response.” (end of quote)
“Conclusions: Poor outcome in the psychological treatment of chronic fatigue syndrome is predicted by variables that indicate resistance to accepting the therapeutic rationale, poor motivation to treatment adherence or secondary gains from illness.”
Predictors of response to treatment for chronic fatigue syndrome RICHARD P. BENTALL, PhD, University of Manchester ; PAULINE POWELL, PhD and FRED J. NYE, FRCP, Royal Liverpool Broadgreen Trust ; RICHARD H. T. EDWARDS, FRCP (retired).
The British Journal of Psychiatry (2002), 181: 248-252
http://bjp.rcpsych.org/cgi/content/full/181/3/248 (end of quote)
“Their use of this phrase reminded me of this : “misinterpretation of associated bodily sensations” (from, Richard Mayou, and Michael Sharpe, Treating medically unexplained physical symptoms Effective interventions are available BMJ 1997;315:561-562) (end of quote)
“Results: Poor outcome was predicted by membership of a self-help group, being in receipt of sickness benefit at the start of treatment, and dysphoria as measured by the Hospital Anxiety and Depression scale. Severity of symptoms and duration of illness were not predictors of response.” (end of quote)
“I’ve met someone who had recovered via GET and CBT, and it was strange speaking to them. They’d say how totally recovered they were, but that a vital part of their recovery was realising that they were not able to do a lot of the things they used to be able to. They now saw their illness as a good thing, having helped them learn to not do too much, where as those who had not been ill would foolishly do much more.
I was rather confused by it all, but didn’t want to push them on it as they seemed a bit fragile. So am I.” (end of quote)
The full article and discussion can be seen here
Quotes from modern research
Another quote from a link provided by Tom Kindlon on Twitter 30-9-13
“Advice to patients from CO-CURE Archives CO-CURE@LISTSERV.NODAK.EDU
NOT: Liverpool CFS Clinic handouts Date: Sun, 29 Sep 2013 07:42:26 -0500″
“the following booklet is part of the Pauline Powell/Liverpool
CFS Clinic oeuvre, which formed the basis of the FINE trial. In it are
yet more examples of ME/CFS patients being explicitly told that a)
there is no organic disease whatsoever occurring in ME/CFS patients,
b) if patients follow the exercises suggested in the handbook/pamphlet
that ‘the symptoms of CFS will gradually disappear’, and c) that
ME/CFS patients’ symptoms following exercise should be ‘mopped up by a
10-15 minute rest afterwards’.
The booklet is uploaded here-
http://www.mediafire.com/?1m6i02ikqxrg78m
p.12 -“As there is no disease it is safe to gradually increase exercise and
activity. But because your cardiovascular system and muscles are
severely deconditioned, and body rhythms are out of synch, graded
exercise is very difficult at first and progress does seem slow.
However, if you persevere with your exercises in a controlled (timed),
gradually increasing way and check your sleep habits, you will build
up your physical stamina and develop a regular sleep pattern. It is
advisable to wear training shoes for exercises.
The symptoms of CFS will gradually disappear.” (end of quote here)
My comment: Many of those recommendations have been directly, or perhaps indirectly copied from my research project of 1982 and essays since. i.e. the author may have read them in the general literature, but they originated with me. However, there are a number of problems that I can see with their version, but since other people are being given the credit for what are essentially my ideas and conclusions, it is simply not worth my while correcting the mistakes
Heated arguments
Throughout more than 100 years of history there has been constant controversy and heated arguments, and even spite, hatred and death threats against people who have different opinions.
The main ones have been whether it is imaginary or real, physical or mental, ordinary tiredness of abnormal tiredness, and whether it is caused by a virus or chemical toxicity, or the adrenal, nervous, or immune system, and since I proved it was physical and involved exercise limitations the arguments centre on whether exercise is good for the patients or doing them more harm than it’s worth.
I set out to solve many of those problems with some success, but now there appear to be people who want to act as if I don’t exist, and copy my ideas and methods to gain the credit for themselves, and they ridicule me and defame my character, and act as if they hate me with a vengeance for accusing them of stealing my ideas, or even for just mentioning that I developed the methods before them, and that they should acknowledge that fact.
Ever since I started I realised that I might not succeed, but what I could do was to describe what happened, and that is what I continue to do.
In the meantime, I have made a lot of advances in the knowledge of the ailment, and developed some very effective methods of treating it, and had a major influence on the course of research.
I wasn’t really aware of how many people were using my ideas and methods until about a year ago, when I saw that Simon Wessely had been given the John Maddox Prize for his contributions to the study of CFS, where he was described as developing “new” methods in from 1987 onwards, and since then I have seen several people claiming that they have had “new” ideas, or developed “new” methods or “new” understandings etc, which they started recently, or ten years ago. or 20 years ago.
There is not much difference between those supposedly “new” ideas and mine, which I developed between 1975 and 1982, more than 30 years ago. However they took me many years of evaluation, and the depth of my knowledge makes a lot of difference.
The Most Common, Complicated, and Confusing Illness in Medical History, including economic and political aspects
|
A quote from another website “Dr. Jesse Stoff Welcomes More Information About Chronic Fatigue Syndrome . . . Chronic Fatigue Syndrome has been a mysterious illness for many patients and doctors over the past decades . . . New York, New York (PRWEB) June 19, 2012 . . . According to Dr. Jesse Stoff . . . Chronic Fatigue Syndrome (CFS), also known as Myalgic Encephalomyelitis (ME) has earned the undeserved reputation as “an alternative wastebasket diagnosis for depression.” . . . According to a recent article in the Wall Street Journal , a new study has been released to reveal more information and treatment options for doctors struggling with how to diagnosis and treat the chronic illness . . . The International Association for Chronic Fatigue Syndrome and Myalgic Encephalomyelitis President, Dr. Fred Friedberg , . . [This condition] affects at least one million people in the US yet up to 80% of them have not yet been diagnosed. Medical providers are often uncomfortable diagnosing and treating these patients and patients tell us that they frequently have difficulty finding a knowledgeable physician . . . The article cites that CFS has cost the American economy loses $18-24 billion each year due to “decreased work productivity, lost tax revenue, increased health care expenditures and disability payments.”. . . Dr. Jesse Stoff hopes this new primer and further immunology studies will not only help patients recover from this debilitating condition, but also help repair the American economy . . . He concludes, “Since the recognition of CFS as a true medical illness by the CDC, research has slowly lifted veil after veil to better understand and treat this disorder”. (end of quote) See here. My comment Throughout history the symptom of chronic fatigue has been labeled as many things which are often given as leftovers when all other possibilities have been tested. Similarly the various labels have been used as diagnosis of exclusion, and of course “wastebasket diagnosis” which means the same thing. It is not the equivalent, or even remotely related to depression which is completely different. In particular chronic fatigue involves “fatigue” whereas depression involves the “mood” of sadness. However, it has been found that about 50% of patients who have chronic fatigue for five years or more develop some sort of psychiatric illness, including depression. That occurs because the patient’s condition is poorly understood, poorly diagnosed, and poorly treated. In many cases the patient is treated like trash with the addition of stigma and prejudice. They are also discriminated against in compensation claims etc. For example, most people with other illnesses will be granted compensation, but the vast majority of CFS patients are denied entitlements to compensation etc. and can’t work, and live in poverty, while those around them are in good health and able to prosper. The cost to the world economy is a lot more than $18 billion, which has a lot to do with the fact that it is ignored and stigmatized. Employers, insurance companies, and governments naturally don’t want to pay those costs, so they are more interested in arguing that the past and current evidence of real illness is not good enough. However, the scientific evidence for the physical basis of the illness already exists. More information on economic aspects can be seen here and here and here. See also my reference number 89 here, by Sanne Kreijkamp-Kaspers et al, an article which discusses the costs of treating CFS in the USA, from Talking Point – the Official Journal of the ME/CFS Australia (SA) Inc. page 8. (originally from the Australian Family Physician 2012). The direct cost of treating CFS in the U.S. with conventional and alternative methods, is calculated at US $2342 to $8675 per patient per year, with indirect cost is $20,000 per year. The inability to work adds to the cost to the patient and the carer, which “equates to a total cost of at least $18 billion per year in the USA alone.” Research incentives and findings Large and wealthy organisations would have a lot of money to spend funding research projects aimed at arguing that CFS is an imaginary, trivial, or psychological problem. If they reported the real basis for it they would have more costs to bear. By contrast patients and do-gooders would have much less capacity to fund research projects to study the real physical nature of the problem.. (When I was being criticised by two anonymous editors in Wikipedia it was obvious to me that they were writing an account of this area of study which favored the wealthy organisations to the detriment of patients.) See also here and here The gradual cause of CFS In some cases people are born with this ailment, and in others it appears to occur after a viral infection, but in the vast majority of cases it occurs so slowly that the person doesn’t know what actually caused it, and neither do their doctors or the researchers. In fact, that is why I began studying it, and it took me five years of thorough detailed observations and notes to identify the subtle and very gradual, almost imperceptible way that the fatigue accumulated. After I established that fact, I was able to recognise the signs of abnormal fatigue in it’s early stages, and prevent the major problems of extreme fatigue from occurring. Consequently, although I still have the condition, I haven’t had the severe exhaustion in the thirty years since. See my report here. However, the following quote comes from the website that I read recently . . .
While it is possible to consider the idea that some sort of stress is the ‘straw that broke the camels back” to cause CFS, it is nevertheless not consistent with the majority of gradual and unknown causes. Also, abnormalities in the nervous or immune systems could also be due to viral infections which are often reported as preceding the ailment. Of course I don’t wish to discourage anyone from doing whatever research they think might be solve these problems. |
The chronic fatigue syndrome is the most common illness in medical history and has been particularly common in the Western World since the seventeenth century when it was recognised as being a disorder of sedentary workers that was rare in farm laborers and non-existent in primitive tribes people.
Nowadays it is commonly encountered amongst patients in every medical clinic and is well known and recognised by all doctors, but there is no generally accepted blood test or x-ray evidence of the cause, and no officially endorsed reliable way of diagnosing the condition, and no consistently effective treatment, and no known cure.
The condition is so complicated and confusing that there are more than 100 diffferent labels for it which vary from one doctor or specialist to another, and from year to year, decade to decade, and century to century, and has often been used as the subject of classroom debates for first year medical students, and sometimes produces heated arguments at medical conferences.
Chronic fatigue was the most common ailment in the nineteenth century when it was called Neurasthenia due to the belief that it was caused by a weakness of the nervous system. That label was the most commonly used diagnosis in medical clinics where the condition came to be regarded as an imaginary, trivial, or psychological disorder. Some researchers thought it was caused by tight corsets which compressed the chest, heart, and lungs. It was therefore known as a women’s ailment but it also affected some men, especially those who wore male corsets, which were common at the time.
During the American Civil War a physician named J.M.DaCost observed the extreme faintness and fatigue in soldiers who had marched into battle with heavy fully laden knapsacks at double quick pace for 16 hours at a time in cold wet conditions, while suffering from an infection. He also noted that the symptoms were ‘undoubtedly’ aggravated by their tight waistbelts, and, as the result of his studies the condition became widely known as Da Costa’s syndrome.
In the early twentieth century when time and motion studies were introduced to improve productivity in coal mines, the condition became common amongst men who were required to increase the tonnage of coal that they shoveled each day to achieve the new and gradually increasing average worker requirements. The illness was then called Industrial Fatigue. However, there was no medical test to confirm the existence of the ailment and that created two problems. Firstly the number of individuals developing the ailment was posing a great cost to industry, and secondly, healthy workers could start faking the condition to avoid their occupational responsibilities, so industrialists socially engineered the idea that it was a psychological disorder, and in Britain the name of The Industrial Fatigue Board was changed to The Industrial Psychology Board. Thereafter healthy workers refrained from faking the condition to avoid being branded as mental cases, and genuinely fatigued patients had to endure the shame and psychological distress imposed on them by the fraudulent defamation of their characters.
In World War 1 the condition affected soldiers who were exposed to round the clock cannon fire in the trenches of the Western Front, where the constant noise made it difficult for them to sleep for months at a time. It also affected soldiers who were exposed to the shockwaves from exploding bombs, but were not hit by shrapnel, so it became known as Shell shock. The undetectable nature of the fatigue again posed several problems for army administrators. Firstly, the large number of cases was reducing the manpower available to do the fighting. Secondly, large numbers of healthy soldiers could start faking the condition to avoid the risk of death on the front line, and the combined loss of manpower could make it difficult to win the war. Thirdly, the cost of military pensions was making it uneconomic to continue the war. The armies therefore started discrediting the idea that the condition was a real physical ailment and reinforced the psychological theories by attributing it to fear, with emphasis on the label of cowardice. Thereafter healthy soldiers would choose to face death in battle rather than fake the fatigue and be branded as cowards, and the genuinely fatigued patients had to endure the shame of the devious defamation. The army chose to conveniently overlook the fact that some soldiers were being granted bravery awards at their bedside while they were being treated in shell shock hospitals. The awards were given to soldiers who demonstrated courage in battle above and beyond the call of duty.
During the Iraqi War the U.S. planes were reported as carrying bombs which were specifically designed to produce the type of shock waves that were most effective in causing the symptoms of shell shock, and many enemy soldiers were reported as being too exhausted to pull the triggers of their guns and were easily captured.
In civilian life some scientists observed that most patients with chronic fatigue spoke of intolerably distressing cardiac symptoms during physical exertion so the ailment was called “The Effort Syndrome”. Others noted the similarity to the normal symptoms of fear and exertion, and therefore concluded that the symptoms may have been due more to the fear of exercise, rather than the exertion itself. However, many of the patients had thin physiques so there was the suggestion that it was due to poor physical fitness resulting from a lack of exercise (some researchers call that ‘deconditioning’ i.e. gradually becoming less and less fit due to the lack of exercise). There were also suggestions that it was due to the fear of competitive sport, or laziness. When the condition affected factory workers who were accidentally electrocuted at work it was called Industrial Shell shock.
Follow up studies from World War 1 showed that the condition was more common amongst lightly built sedentary workers who were sent off to war without the proper amount of physical training, and they were expected to keep up with the marching pace of solidly built soldiers recruited from farm laboring communities. Consequently, by the start of the second World War, volunteers with such physiques were rejected on medical grounds. However, even the fittest of recruits could develop the fatigue if the conditions of war were severe enough. Their condition was called Battle Fatigue. Prisoners of War who lost more than one third of their body weight due to starvation developed chronic fatigue and many of them were still troubled by abnormal fatigue thirty years later.
Some psychiatrists continued to believe, or promote the idea that the absence of blood test or x-ray evidence of disease was an indication that there was nothing physically wrong with the patients, so they diagnosed the condition as Anxiety State, and other psychiatrists noted that many of the patients with chronic fatigue were depressed so they called it a Depressive Disorder, but most doctors reported that there were patients in almost every clinic who had the condition but appeared to be as anxiety free and as well adjusted as any of their other patients. When the condition affected a soldier at war some psychiatrists continued to attribute it to the fear of battle and called it Battle or War Neurosis, and if it affected a person at work they attributed it to laziness or psychological stress so they called it an Occupational Neurosis, and if the person claimed workers compensation for the ailment they believed that the motive was subconscious greed so they called it Compensation Neurosis, and they believed that after the workers left their employment or received a large financial payout from an insurance company they would make a rapid recovery. Those psychiatrists did not do proper follow up studies, because they were not aware that many patients were forced to resign without the benefit of workers compensation or other entitlements and spent the remainder of their lives in poverty.
Furthermore, by not informing workers of the consequences of continuing to work while in a state of fatigue they were neglecting their responsibility to provide preventive advice, and contributing to the development of the chronic condition, and hence were contributing to economic costs to the patients and society.
(It has been a feature of medical history that obscure illnesses have been prejudically attributed to negative, rather than positive personality traits, such as evilness, sinfulness, laziness, cowardice, or greed.)
After more than 100 years of the condition being popularly attributed to laziness or a fear of exercise, it became widely known to affect Olympic athletes, Sports Champions, Football stars, Marathon runners, and World Record holders. The new profession of sports physicians attributed it to excessive physical strain without adequate rest breaks, and began calling it the Overtraining Syndrome. For example, if poorly prepared athletes participated in too many marathons in the one year they were likely to develop chronic fatigue. They didn’t have sufficient time between marathons to fully recover, so when running each additional marathon they just compounded the fatigue which permanently impaired their fitness capacity until they could no longer compete at the elite level, and in the worst cases could not continue with normal employment or lead normal lives. (i.e. it was caused by overwork amongst athletes who were enthusiastic about exercise). The sports doctors recognised its chronic nature and the fact that it could ruin the careers of professional athletes, so they began recommending graduated and regulated physical training programmes as important methods of preventing and treating the problem.
The condition is also common in pregnancy and in other cases it persists or starts after childbirth when the post-natal fatigue has been called Post-Natal Depression, due to the belief that it is the result of the psychological stresses of motherhood. Some women with chronic fatigue can trace their first experience of fatigue back to a pregnancy which may have occurred twenty years earlier, and that prior to the pregnancy they were fit and healthy and had a lot of energy and played a lot of sport.
Other patients report that they can trace the condition back to a traumatic experience in their past, such as the death of a spouse, or the break up of a relationship.
Throughout history there are many examples of epidemics of chronic fatigue of unknown cause which have occurred amongst localised communities such as an outbreak in Akureyri in Iceland in 1948. The symptoms included headaches, sore throat, muscle pain, spasms, paralysis, tiredness, and emotional instability. This set of symptoms was called Icelandic Disease to identify it’s locality, with a medical diagnosis of Myalgic Encephalomyelitis, and it was thought to be due to a contagious viral infection. In some cases the fatigue persisted for weeks or months or even years afterwards, and the duration was related to the extent of the paralysis during the original phase. It has been proposed that the persistence of fatigue was due to a post-viral condition where the virus became dormant or hidden and produced long term strain on the immune system. In 1955 there was an outbreak of the ailment affecting 300 of the male and female staff of the Royal Free Group of hospitals in Great Britain where it became known as The Royal Free Disease. Also, after a flu epidemic in Tapanui, New Zealand, many patients were left with persistent fatigue which became known as The Tapanui Flu.
In World War 1 60,000 British soldiers returned from the trenches of the Western Front where they were exposed to the cold and wet, poor nutrition, blood, pus, rotting corpses, bed lice, contaminated food, food poisoning, dysentery, and wound infections, and the war was finally brought to an end by the Spanish flu which killed millions of soldiers and civilians and was the most severe influenza epidemic in history. After recovering in hospital from months of dysentery and flu the fatigue persisted and many veterans continued to suffer from fatigue for the remainder of their lives.
There are also many cases where patients who have had chronic fatigue for many years, can trace the onset of their condition back to a viral infection of some sort, such as Glandular Fever. Prior to that infection they were fit and healthy and lead normal lives, and since then their lifestyle has been restricted by the fatigue.
Other patients report that they can trace the start of the fatigue back to a period of exposure to farm insecticides, or factory chemicals.
Some patients report that is has been a problem since they were born because they cannot remember a time in their lives when they were not easily fatigued, and others cannot recall any particular starting point or incident, and some say that the condition seemed to start incidiously for no identifiable reason and that it gradually got worse until it affected their sport, and then their social life, and ultimately their employment.
There is evidence of a disorder of blood flow throughout the body so North American medical researchers called it Neurocirculatory Asthenia, and Russian researchers called it Vasoregulatory Asthenia based on the idea that it is due to a disorder that affects the regulation of blood flow.
Apart from the fact that the actual physical or organic cause of this ailment has not yet been found, the other reason for the condition being confusing is that there are probably several different disorders being diagnosed as one. For example, some of the conditions may be sleep disorders (related to tiredness) and some may be exercise disorders (related to physical fatigue), and others may be a combination of sleep and exercise disorder. There may also be several different causes for each type which have the same ultimate affect on the body.
In the nineteenth century the condition was commonly seen in women who wore tight waisted corsets which compressed the chest, heart, and lungs and impaired blood circulation from the feet to the chest and brain.
According to The Posture Theory, poor posture compresses the chest and abdomen, and sedentary work involves repeated or constant leaning toward a desk, and when both of those factors are combined the heart, lungs, and abdomen are being repeatedly compressed, and if that process is continued for many years it can eventually and permanently affect the the blood flow from the feet to the chest and brain, and the regulation of physical responses to exertion, and sleep patterns, which is characteristic of The Chronic Fatigue Syndrome.
Multiple factors need to be considered when assessing the cause, and the type of CFS. M.B.
The possibility of many causes
Some people have argued that coronary heart disease is due to genetics, cholesterol, smoking, alcohol, stress, or worry, and or combinations of those factors. All of those suggestions may be correct.
Some people have argued that the chronic fatigue syndrome is due to genetics, excessive and prolonged exertion, overwork, viral infections, disorders of the immune system, or the autonomic nervous system, exposure to toxic chemicals, postural problems, stress, or worry. Probably all of those factors are correct.
Unfortunately, people who favor one idea, generally try to argue that everything else is wrong, regardless of the fact that they can’t prove their own idea, or prove that the others are wrong.
Overwork or laziness as the cause of CFS?
and “Conflict of Interest” in research results
The most logical cause of the chronic fatigue syndrome is that the person works too hard, beyond the limits of human endurance, and hence fails to recover, and remains chronically fatigued. For example, they may work long hours for many years, or go on long marches with heavy knapsacks for weeks at a time while poorly fed and suffering from infections, or they may participate in too many marathons without sufficient rest in between.
However, research into cause is funded by people who have money, such as large companies, and they want ideas aimed at keeping their workers healthy and productive. If they can’t get that result they want ideas which enable them to save the costs of illness, such as compensation and pensions.
Therefore they tend to favor the ideas which blame the patient for the problem and make them appear as if they don’t deserve compensation etc.
Hence the ideas that get the most publicity are those which argue that the patient isn’t actually ill, or that the evidence of real illness doesn’t exist, or if it does, they deny it, or hide it, or argue that it isn’t good enough. There are also arguments that the patient is imagining things or that the symptoms are trivial, or that the person is just complaining to get sympathy, or that their fatigue is due to laziness and the lack of exercise, and that they don’t deserve compensation or insurance payouts etc, and that all they have to do is think positive and exercise regularly and their symptoms will disappear.
It has even been argued that as soon as the patient gets compensation their illness miraculously disappears. However, long term studies show that the condition remains chronic regardless of whether they get insurance payouts or not.
The fact remains, that it is much more logical to suggest that overwork is the cause, or at least one of the causes, and that laziness and lack of exercise is not. For example the world is full of people who are proud of the fact that they never exercise, and the ‘couch potatoes‘ who watch TV all day, but despite the complete and utter lack of exercise they are still in perfect health.
The idea that the symptoms are due to laziness, or mental weakness, or poor character etc, is an advantage to large companies because it creates prejudice against the patients, and leaves the public impression that they don’t deserve compensation etc, and acts as a sort of justification for not paying the same entitlements which apply to other illnesses.
Of course patient groups do try to raise money to fund research projects, but in their state of ill-health they have difficulty raising the funds, and can’t compete with the financial clout of the large companies.
Hence while the majority of patients will tell you that their symptoms are abnormal and physical, and while there is a massive amount of scientific evidence to support that view, the prevailing opinion of laziness or mental cause reflects the influence of the large companies and organisations who have the most money available to fund the research.
Patients need to understand such influences on the ideas about their illness and not just passively complain about how unfair it it. They need to do something in an organised way themselves.
(Nobody would argue that cancer is caused by laziness so it is somewhat curious that anyone would believe that the chronic fatigue syndrome is caused by laziness).
Financial incentives in research opinions
If a large organisation such as the tobacco industry offers financial assistance to scientists to do research into the health problems caused by smoking it is likely that most respectable scientists wouldn’t accept the money because the cause and effect relationship is obvious. However some incompetent academics would see it as an opportunity to make money the easy way. They would know that if they found proof that smoking was the cause of cancer the information would be covered up, and their funding would be stopped. They also know that if they could construct a study to show that it was not the cause the funding would be likely to be renewed each and every year in the future. They also know that they would be likely to get increases in funding and promotions to put them in charge of other staff to ensure that those who found the same results would be retained and promoted, and those who found proof of cause would be demoted to a position of insignificance or sacked.
Hence if anyone found proof of the cause and effect they would be described as fringy kooks who were foolishly challenging the official opinion of internationally renowned and prestigious researchers.
The same general paradigm affects any organisation where the illness presents financial or other liabilities and costs, including the chronic fatigue syndrome.
See also here and here and the costs of CFS here.
Some Extreme Medical Attitudes about so called laziness, and irresonsibility in CFS
On 15th November 2013, Tom Kindlon posted a tweet about another letter tweeted by richardcann76 here, which was about patients with the chronic fatigue syndrome. Richardcann76 presents some valid complaints about the professional misconduct of a doctor called Dr.X who has been saying some very derogatory and insulting things about CFS patients.
For example, he says this about Dr.X. . . “A search of his past BMJ posts suggests that he has a pretty low opinion of his patients, particularly those with long term, chronic illness on state benefits, who he suggests would be better off “with a report from their social worker for their assessment of their ability to work. . . . and . . . “because it gives me (Dr.X) the opportunity to start a discussion on how they can improve their lives through work rather than wallow in worklessness . . . and he considers that the patients just have . . . “a mixture of mild organic problems, moderate emotional difficulties and severe social disincentives (to work).
The attitude of Dr.X is that the patients are just complaining about illness to get secondary gains such as ” attention” or, “financial” benefits, “or simply to find an excuse to wallow in worklessness or avoid life’s responsibilities”.
My comment . . .
Any person who researches the ailment properly will find thousands of research papers about physical and physiological abnormalities which explain the symptoms, and can see follow up studies which show that it has long term consequences.
In other words, any patient or doctor or medical authority who studies this ailment will know that Dr.X is not just an ignorant fool, but is a liar who should be permanently banned from any profession which treats patients, and put in jail.
The letter by richardcann76 can be seen again here.
My final remark is that Dr.X is also incompetent in his understanding of CFS and would be completely and utterly useless at treating it and would cause his patients a lot more harm than good.
Eliminating criticism of Diagnostic Criteria for CFS
One of the problems in research is getting specific results which are confused with other factors, where some people have falsely argued that the symptoms could simply be due to a lack of exercise, or depression etc.
Hence, if I was to do a fitness study again, I would ensure that the selection criteria eliminated that confusion in the following manner.
1. The patients should have a type of fatigue which restricts their capacity for strenuous exertion and involves measurable abnormal physiology which is evident as the level of exercise increases, or afterwards.
2. The individuals should report that they have to occasionally take forced deep breaths where they often feel as if they cannot get as deep a breath as they need, and hence may take a series of two or three forced breaths. This is due to inefficient respiratory function, and is more likely to occur with greater frequency during exertion.
3.The individual should have a history of being physically fit and involved in strenuous sport in the years prior to developing CFS.
4. The individual should not show any signs of sadness, gloominess, or despondency, or any other psychological evidence of depressed mood. The history of research clearly shows that such individuals do exist and are not particularly difficult to find.
Once the data of the fatigue has been clearly determined, then it can be reassessed in relation to mixed groups later.
What not to do – Don’t mix the study with people who have never exercised or played sport in their life, or individuals who look and act miserable and despondent, or you will get mixed results, and your critics will argue that they are all just unfit due to a lack of exercise, or are all depressed, and that your results and conclusions mean nothing.
|
I considered all individuals with chronic fatigue. Modern definitions tend to focus on a narrow range of symptoms and call it ‘The Chronic Fatigue Syndrome’ which gives the advantage of gaining consistent data, but creates the problem of excluding all other types from being called by that name. They are all different types of ‘chronic fatigue syndrome‘, and all need to be identified and studied. The common problem is fatigue which restricts activity and lifestyle. Consider this reference from 1950 before that label was used . . . Wheeler E.O. (1950), Neurocirculatory Asthenia et.al. – A Twenty Year Follow-Up Study of One Hundred and Seventy-Three Patients., Journal of the American Medical Association, 25th March 1950, p.870-889 (Contributors to the study: Edwin O.Wheeler, M.D., Paul Dudley White, M.D., Eleanor W.Reed, and Mandel E.Cohen, M.D.) |
Chronic fatigue syndrome and Varicose veins
. . . and why my critics are so hostile and want to hide my existence and my ideas
re: varicose veins in the legs cause slight faintness, chronic fatigue involves more faintness – and the reason why
|
Varicose veins in the legs are larger than normal veins and take longer to fill, so the blood going down from the heart to the feet takes slightly longer to get back to the brain. That feature is called Delayed Orthostatic Hypotension, and is an occasional cause of faintness. |
When I began studying medicine I had so many symptoms that I was told that the only possible cause was a disorder of the mind because it was housed in the brain and attached to every part of the body by the nervous system. I was further told that no other factor connected all parts of the body together and that no other cause was possible.
However I soon established that poor posture, and leaning forward could compress the stomach to cause stomach pain, and compressed, and compressed the ribs to cause chest pains, and the lungs to cause breathing problems.
I also knew that leaning forward had induced a sense of faintness which had been relieved by sitting upright, and suspected that poor posture could also be the cause of fatigue but I didn’t know how, and started looking for other factors.
Four years later, when I found out about Valsalva’s maneuver I was soon able to determine how poor posture could compress the air in the chest, and hence the blood vessels in the chest, to slow the flow of blood between the feet and the brain produce a tendency to faintness and fatigue (poor concentration and tiredness), and well as a reduced capacity for exercise.
I therefore had to determine why the tendency to faintness and fatigue had become chronic and related to many factors other than poor posture.
I therefore came to the conclusion that compressing the air in the chest repeatedly hundreds, if not thousands of time per day while doing sedentary work, could have strained or stretched all of the blood vessels below the chest, or made them weaker, so that they tended to stretch more easily than usual. Hence they were either larger in size, and had a greater capacity for blood than normal, or were prone to stretching which would give them that greater capacity.
Hence, in such circumstances, the blood coming down from the heart would take longer to fill them, and there would be a slight delay in its return to the brain.
That delay, or the weakness or inefficiency of blood flow to the brain would explain the chronic nature of fatigue.
I then decided to help people understand my theory by providing example of which part of the vascular system had been weakened.
It could damage to the muscles or nerves in the walls of the arteries, or the veins, or the fine capillaries between them, or it could be due to damage to the neurological reflex centres which co-ordinate, and try to normalise blood flow.
The example which I chose to use as on of countless possibilities was damage to the large abdominal vein called the inferior vena cava which brings blood from the two leg veins to the heart.
Many years, or decades later I was looking into the topic of Varicose veins, which are generally leg veins which have become stretched and enlarged by such things as leg garters which blocked the upward flow of blood and caused the one way valve below to give way and the veins to dilate and widen in a manner that is lumpy and curved and twisted.
The quantity of blood which those dilated veins contain is much larger than normal. I then saw a comment that they take longer to fill than normal blood vessels so that some people with varicose veins feel a slight sense of faintness when standing up suddenly.
I also found that another name for the Chronic fatigue syndrome, is Orthostatic intolerance and that there is evidence that the symptom of faintness is related to a scientifically measurable delay in the return of blood flow to the brain.
I therefore, of course, concluded that people with varicose veins have slight problems with faintness because their veins are slightly larger than normal, and that chronic fatigue patients have more obvious problems with faintness because a much larger area of their blood vessel or vascular system is affected.
If you follow what I have just explained than you will know that it is a very logical, sensible, and evidence based concept which is perfectly reasonable, and at least as good, if not better than any other theory that has been written on the subject.
However, while i have actually solved the problems of many patients by presenting a very credible explanation of a physical cause of symptoms, I have unfortunately created discontent and offense to some of those who have been arguing in the past that they symptoms are “all in the mind”.
When the general public see the criticism of me and my ideas they are having their attention focused on the supposed faults in my personality, or my ideas, to divert attention away from the motives of my critics who don’t want people to think that their ideas may be wrong.
One such individual was an anonymous editor of Wikipedia, who was not just criticising me in a “proper” or “normal” manner, as required by the rules, but was insulting, belittling, ridiculing, and mocking me in a hostile and offensive manner, and nitpicking almost every word I wrote for 12 months, and deleting it, and the evidence at every opportunity, and did not stop until I was banned.
An example of absolutely ridiculous nitpicking by that editor can be seen here.
An example of that editor co-operating with another to discredit me can be seen here.
An example of the words used to get me banned are quoted below . . .
“I think that a broad topic ban (including Da Costa’s syndrome, Chronic fatigue syndrome, Varicose veins, and any articles even slightly related to human posture, fitness, or fatigue) is an appropriate outcome. WhatamIdoing 20:25, 27 January 2009 See here, and two of my reports here and here.
More of my reports on varicose veins can be seen here and here.
My reports on Valsalva’s maneuver and faintness (due to pressure on the air in the chest) here and here and independent evidence for that pressure here.
More than one factor connecting every part of the human body
I also determined how poor posture could strain the spine to cause neck and back aches, and alter the angles of most skeletal and internal structures to cause such things as kidney aches, sore throats, and jaw pains etc
I had therefore proven that there were at least two possible factors connecting every part of the body together, with the skeletal system being the other one, and that therefore there were probably many possibilities which had, or had not previously been considered.
My critics are offended, spiteful, vindictive, and hostile because I have proven that their claim of only one possible cause is wrong, and I have proven a physical cause, to replace the old ideas of psychological cause.
I expect them to continue in that manner, and they will “possibly” be successful “socially”, but not “ethically”, or “intellectually”.
My response to the letter of Dr. Dairymple’s
In 1975 I had many health problems which were not responding to any form of medical treatment, so I decided to study the matter myself.
To describe that task as difficult would be an extreme understatement. See why I started here.
Firstly I spent most of my time laying on the lounge room carpet, because that was the only position I felt reasonably free of pain or fatigue, and I could think for many hours without problems. However, when I sat up and leaned forward to read or write I would have to deal with a lot of abdominal pain, so I would learn the medical language at the rate of one word per day, and write small sentences at a time.
I joined an exercise class and was always running last in a class of 50 or more, but that didn’t stop me.
When I wrote essays there were some people who would argue that if I could do that, I wasn’t in pain, and I should be able to get a job, but there were others who criticised my obviously “different” style of writing in “sentences” and paragraphs” instead of “paragraphs” at a time, instead of pages and chapters etc.
It took me four years to determine why I was always relapsing into fatigue, and it hasn’t happened since I learned how to control it. It took me five years to write my theory connecting all symptoms to my spinal shape, posture, and physique, and it was at least ten years before I felt even remotely healthy. It then took me another eight years to determine how to prevent the abdominal pain.
During that time I also had one period of six months of angina heart disease which I treated with a vegetarian diet, and six years of Non-Hodgkin’s Lymphoma, CHOP and DHAP chemotherapy and a stem cell transplant, and four years of side effects.
The older I get the more detailed my understanding of disease becomes, and the better I get at managing highly complex health problems and their interactions, so I actually now have reasonable health, although with many limitations.
When I joined Wikipedia one of their anonymous pathological liars made the snide remark that ‘given the amount of writing I have done, for me it is not a trivial thing”.
The fact is that most people with chronic fatigue can’t do much, and those who do, against considerable difficulty, are treated with contempt.
Another example of that ridiculous and offensive attitude is that of an anonymous doctor who gives the fictitious ID of Dr. Dairymple can be seen below.
The only words in her rant are the admission that her own opinion is “admittedly rather ill-informed”.
She also says that, in her opinion, “the unwillingness of the medical profession to speak plainly on this matter is a sign of pusillanimity, not of obduracy.”
I will therefore speak plainly about Dr. Dairymple . . .
You show extremely bad judgmenta by giving such strong opinions about something that you admit to being “ill-informed” about.
You are a useless and worthless menace to patients and should be permanently banned from the medical profession and never again allowed to make money by treating them.
Note: Dr. Dairymple refers to the fact that her patients had consulted many doctors in the past to get help. She was the 46th.
I probably consulted more than a dozen doctors over a period of five years, and was sent to many x-rays and blood tests, and prescribed countless numbers of pills, potiens, and capsules, before deciding that I would have to take on the responsibility of solving the problems myself.
Dr. Dairymple’s Letter
“A short time ago, I published an article about myalgic encephalomyeltis. I broke no new scientific ground: I merely suggested that the condition was akin to neurasthenia or old, and – unlike real diseases – was more common among the semi intellectual middle classes.
To my surprise, I received scores of letters from sufferers: despite the fatigue which has prevented them from going to work, washing up, shopping and so on, they managed to write several pages of impassioned prose.
I went to a symposium on the illness (if that is what it is) last week. As the participants gathered just before it began, I heard anxiously whispered questions among them as they tentatively sounded each other out: ‘Do you believe in it?” Care had to be exercised, because two sufferers were in the audience, pale and thin-lipped ladies of vengeful appearance, waiting to pounce neurasthenically on those who dared to suggest their sufferings were other than virally induced.
From time to time I see cases of this mysterious condition, and in my heart of hearts I believe it to be a sickness not of the body but of the spirit. I am rarely the first doctor the sufferers have consulted: more frequently I am the 46th.
The patients come armed with sheaves of papers, pamphlets, documents and so forth to persuade me that there was never suffering like theirs, and that it is viruses that cause it. The whole episode is more like an attempt at religious conversion than a normal consultation.
‘What’s your position on ME? they say, more like an accusation than a question. ‘I don’t think ME is incompatible with a long life’ I remark, as mildly and dryly as I can.
Quite often I am handed a photcopied page of laboratory results, in the way that candidates for rather minor positions hand over educational certificates or personal testimonials. The results are of antibody tests ordered by doctors convinced of the reality of ME (by reality I mean, of course, the physical causation).
The antibody tests demonstrate that at some time in the past the patient has been infected with one or several viruses. The presence of these antibodies reinforces the conviction of the patient that he or she has an indubitably physical illness.
In vain do I tell the patients that my blood carries antibodies against hepatitis A, but this does not account for the tiredness against which I – like most of humanity – have long struggled. Koch’s postulates are not fulfilled by the mere presence of antibodies (or even of the allegedly causative virus themselves). Until some can demonstrate that viral infections produce the same effects in a population that has never heard of ME, I shall remain skeptical.
By now, it will be obvious to the reader that I do not have a completely open mind on the subject. . It is an escape route for the middle classes, especially teachers and paramedics such as physiotherapists, occupational and speech therapists.
I do not in the least blame them for wanting to escape. Anyone who had dealt with modern British youth or the public at large must often want to do that. But the desire to escape is not something they can easily admit to themselves, especially if they see themselves carers (horrible word).
ME offers not just an escape but something better still: a cause. You can suffer and, by joining one of the pestilential self-help or pressure groups, believe that in some way your suffering is not entirely in vain, but it is helping to bring about a better world.
Almost everyone I spoke to at the symposium agreed with me, but only in secret and only in hushed tones. Of course, the ME groups will take this as yet another sign of the medical profession’s criminal blindness and lack of understanding (how delicious it is to be misunderstood by everyone!) But in my opinion, the unwillingness of the medical profession to speak plainly on this matter is a sign of pusillanimity, not of obduracy.
My experience of ME sufferers is that they suffer triumphantly, and that their claim that the disease has ruined their lives is not to be believed. I could write a great deal more on this fascinating subject, but unfortunately I had the flu four years ago and am feeling rather tired.
Theodore Dalrymple is the pen name of a practicing doctor. 28/Medical Monitor/14 February 1992.” See one of the sections on the website here.
Former Olympic athlete Raelene Boyle
was misdiagnosed as having panic attacks and chronic fatigue
On 14th September 2012 the channel 9 TV show called “A current affair”presented an interview with former Australian Olympic athlete Raelene Boyle who described how she had previously been misdiagnosed with panic attack in 2000. She would often feel faint before giving public talks or when walking her dog, and have to stop to lay down to relieve the symptoms. However, earlier in her life she had been in situations of stress and didn’t think that it was possible for her symptoms to be due to stress or panic in such minor situations as walking her dog. She also suffered from fatigue and was tired and would sleep for up to 20 hours per day.
More recently, after having those debilitating problems for about 12 years, a doctor diagnosed that she had artrial fibrillation of the heart, and she had surgery to implant a pacemaker. Since then she has not had any symptoms and has been able to return to normal activities for a woman of her age of 61. She said that she hadn’t felt so healthy for many years.
My comment: Many CFS patients will report that they get chest pains and other symptoms for no apparent reason when there is not stress or any other obvious factor to account for it, and the same applies to their chronic fatigue. It is just a feature of their health that has nothing to do with stress or panic. See also here.
Why I was invited to design a research project to study chronic fatigue and exercise at the South Australian Institute for Fitness Research and Training in 1982
|
Summary of my talk 1. As a teenager I played a lot of sport and present 2 photos of gymnastics to show some examples. 2. At age 25 I developed exhaustion for other reasons, and it wasn’t responding to medical treatment. 3. I therefore joined a fitness class to gradually improve my capacity for exercise, and continued for ten months. 4. A few years later I read a book which reported that researchers were having difficulties studying the effects of exercise on chronic fatigue because the patients “could not or would not train”. 5. I later met the head of the fitness research institute and told him that I already had trained in his organisation, and that other people could and would train if they did it my way. 6. His researchers were busy on other projects so he asked me to design and co-ordinate a research study myself. 7. I arranged for a newspaper article to be published inviting fatigued patients to join, and show a photo of the article. 8. The programme proceeded for 12 weeks and another news article reported the success of the project, so I show a photo of that article. 9. The second program proceeded and it’s success was reported in state and interstate newspapers, so I show a photo of one of them from the West Australian. 10. In the next few years I heard a radio show report of a “new” disease called the chronic fatigue syndrome, and I knew that it wasn’t new, but just another label for the same ailment that I had been studying. 11. Recently I have learned that a London doctor named Simon Wessely has been awarded prizes and a knighthood for his contributions to medicine, which included chronic fatigue syndrome as his main interest.. 12. My review of his biography shows that he began his study of chronic fatigue syndrome in 1987, and developing a “new” treatment called graded exercise therapy, but it uses the same principles that I had developed and scientifically proven at the SAIFRT in Adelaide, three years earlier. |
Part 1


Examples of my gymnastics experience when I was a teenager
When I was young I learned to swim at local beaches, and spent many years involved in sport and gymnastics. See here.
(The first photo on the right shows me doing a front somersault off a one wheel bike called the ten footer. It was actually 9 foot six inches from the base of the wheel to the seat. My feet are 12 feet in the air as I am halfway through the somersault rotation. At the top of the photo you can see the corner of the ceiling of the gym hall which was in a 2 story building. The man standing in the audience on the far left near the back wall is my father. He is looking casual, and was treasurer of the gym club, and later a president of the Edwardstown RSL. The other members of the audience are looking worried about the prospect of me falling on them. The 2nd photo shows me doing a straddle jump where my head is ten feet from the ground after a brief run up and bounce from a six foot long spring board. Notice the smile on my face, indicating that I enjoyed gymnastics).
However, by the age of 25 I had acquired many health problems, including exhaustion, for other reasons, and my doctor was unable to explain the cause, or treat them effectively, and that had been the case for several years.
I therefore decided that I would have to solve those problems myself so I began with the idea that I could start exercising at a low level, and gradually improve over a period of weeks, months, or years if necessary, until I became fit and healthy again.
At around that time I heard about an organisation called the South Australian Institute for Fitness Research and Training, so I made some enquires, and found out that it had exercise classes which anyone could join.
I therefore enrolled and then the first thing that each person was required to do was to undergo a medical examination where they were placed on a stationary exercise bike, and had several wires attached to their chests by suction cups with the other ends connected to medical testing equipment such as cardiographs. They were then asked to peddle for 3 minutes, and rest, and then a measured pressure was applied to the brake and they were asked to peddle for another 3 minutes, and then rest again, and the pressure on the brake was increased each time through several phases. The information of load over pulse rate etc, was used to produce graphs which gave a scientifically accurate and reliable calculation of their aerobic capacity, which is essentially their fitness level.
Soon after that I started attending the exercise classes which were conducted twice per week for an hour each time.
Each class began with 20 minutes of light exercises, followed by floor exercises which included pushups. However, while each person was asked to do about 20 pushups I could only do 2 or 3, and was not able to do them properly. That session was followed by 20 minutes of walking or running along a 400 yard track around an oval. However, I could only walk slowly, and when I started jogging I would soon need to stop to get extra breath, but I continued to stop and start at that slow pace as all the other runners out lapped me. We then had another 20 minutes of various activities.
At that stage, where I was coming last on the field, I had to decide what to do, and I only had two choices.
i.e. Go back to my doctor who didn’t understand the problem and couldn’t treat it, or continue with the fitness sessions with the view to very gradually increasing the level of activity and returning to my former capacity – so I kept training.
I gradually increased the pace of my walking and jogging, but it was still slow and intermittent, and I gradually increased the frequency of exercise from twice per week with groups at the institute venues, to three times per week, and then to an additional 1, 2, and 3 times per week on my own at local ovals, or six times per week in total.
I kept training in that manner for about ten months when I injured my knee cartilage and had to stop.
At the start each person was given a card where they recorded the date they trained and their pulse rate etc. One of my cards, from the last few months of training, showed that I trained 5 times in a 10 day period, or once every second day, but I probably trained more than that but did not record it every time I trained on my own.
In the meantime my general health had improved somewhat, but not to the extent of normal health, and I had my aerobic capacity measured at least three times.
At the outset, when my aerobic capacity was first assessed, the level was so low that it couldn’t be measured properly, and was recorded as zero. After 3 months of training it had increased to 350 kp’s.
A form provided by the Institute has it’s letterhead and shows that information signed by, assumedly, one of the research cardiologists, with the comment “V good improvement allround”. Other information appears to have been added by me as notes, and shows that at the next medical assessment my fitness was measured at 350 kps indicating that I had a physical limitation which did not improve any more despite the increased activity and frequency of exercise. The notes also show for comparison that a friend of mine, the same age, who played sport on Saturday mornings and trained on Wednesdays had an aerobic capacity of 900, and an athlete at the olympics would be 1200 or more, and a sedentary worker who did no exercise 700, and a 40 year old overweight asthmatic who I met there had a capacity of 600. In other words my level was about half normal.
After I stopped training I continued to try and improve my health by studying the ailment, and began by buying a small Readers Digest book called The A-Z of medicine (or something similar), and by reading one word a day I found the name of Da Costa’s syndrome where the symptoms matched my own.
I then started reading books of anatomy, and then gradually learning the medical terminology, and after a few years was reading medical reference books and research journals.
I then came across a book which suggested that when patients with that condition were young they had been protected from the hazards of sport by their overly cautious mothers, and had therefore never been involved in physical activity, and hadn’t developed the normal fitness or stamina of other boys, and consequently, as adults, they were easily exhausted by effort, or had a fear of exercise. That book, published in 1956, was by Paul Wood, Britain’s top authority on the subject, and had a major influence on world opinion for the next 20 years.
A year or so went by when I found another book which said that the people who were trying to do research into the effects of exercise on chronic fatigue were not able to do so because the patients “could not or would not train” in the prescribed manner. The comment “could not” referred to a possible physical cause, and the additional remark, ‘would not” referred to the idea that the patients could exercise if they wanted to, but that they refused to train, or were afraid to train,
I knew that the symptoms were not due to the lack of exercise, or the fear of exercise, and that it was possible to train because I had previously done it all myself.
Several more years went by when I met a friend who I hadn’t seen for a long time, and discussed those matters. He said that he knew Tony Sedgewick who was the head of the fitness research institute, and recommended that I tell him about it.
I then phoned the institute, and was invited to a meeting where I discussed what had happened.
I also mentioned that he could verify the facts by checking his own organisations records from 1976 because my file, with my results, would still be there.
I then suggested that if his researchers organised the exercise program the way I had, that they would be able to get as much scientific information about the ailment as they wanted.
Essentially, the objective was to test people at the start, train them for 12 weeks, and test them again to scientifically determine the effects of regular exercise. However, where other researchers were expecting the patients to increase the pace and distance traveled each week, some would drop out in the first or second week etc, and none would be left to test 12 weeks later. I suggested that they would train for that period of time if they were asked to continue, and improve at their own rate, and within their own limits, and then some of them would still be there 12 weeks later, so It would be possible to test them and determine the effects.
He agreed and said that he would discuss it with his research staff.
I phoned him again a few weeks later and he invited me in for another meeting where he explained that his researchers were too busy on other projects. I was about to get up and leave when he said . . . “Why don’t you do the research yourself, since you know more about it than anyone else”.
If I was healthy I would have thought that was the best offer I had ever had in my life, but I explained that I still had health problems which would make such a task difficult. I also said that I didn’t have any medical qualifications, and didn’t know how I could be authorised to do such a project, and I didn’t know how to write research papers, and that a medical journal probably wouldn’t publish a study by a non doctor.
However, he said that I had qualifications in organising groups and that I could set up a committee, and that he would be on it, plus me which would make two, and that he could arrange for his two research cardiologists to do the medical testing, which would make four, and that he could give me the names of doctors who were interested in doing research, and that I could contact them, and would only need two more to produce an officially approved research team. I said that I would also need an experienced instructor who would understand and be willing to run the exercise program according to the specifications required, and he said that he knew several people who he could ask to do that.
I told him that I would think about it and let him know.
Over the next few weeks I kept telling myself that I shouldn’t commit myself to such a task, but ultimately I thought that if I didn’t do it, that no-one else would figure out what to do for another 100 years, so I arranged for another meeting where I agreed to do it, and the process began.
Part 2
At that meeting I was given information about what was required to set up the project.
I needed to contact a politician and apply for funds to gain official government authorisation, and then find two other medically qualified people to join the team, and I wanted to meet the instructor to assure myself that he understood the aims and specific methods involved.
In other words I wanted that person to understand that we were not trying to create athletes, but needed them to train in their own way, at their own level for 12 weeks. If we couldn’t do that we were wasting out time.
We also needed to recruit individuals to be tested.
I then sent a letter to a politician and attended an interview and later received a letter offering a small grant. The amount was just a token payment but it gave official approval for commencement.
I phoned and met several doctors who were interested in co-operating with a research project, and found one general practitioner, and one psychiatrist who were willing to join.
I met the instructor and found that he had university qualifications, and an interest in fitness, and experience in other exercise programs studying various health problems at the institute, and that he understood the objectives. He was ideal for the course.
We then needed to recruit people to do the training.
The head of the Institute arranged for anyone who enrolled in general classes to be assessed to determine if they were relevant to the fatigue program and directed them to it, and at one stage a letter was sent to general practitioners advising them of the program.
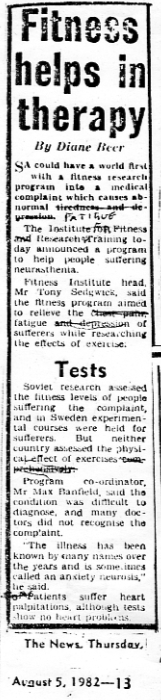
![]()
In the meantime, I contacted a medical editor of the afternoon newspaper called the “News”. The editor phoned the head of the institute to confirm the details and then published an article to invite people to attend.
The first article reported the announcement by the head of the institute of a possible world first study, with me as the research coordinator giving information about the type of ailment and inviting people to join.
Essentially, by that stage, everything was set up, and then proceeded as planned.
I then waited for three months, during which time the initial medical testing occurred, and the course of exercise training began, and continued to the second stage of testing. I then collected the files containing all of the information, and extracted the details, and prepared a report.
I then arranged another meeting with the head of the institute, and advised him that our objectives had been achieved.
In particular, that if the exercise principles which I defined were used then the patients “could and would, and did train” for sufficient time to gain scientific data on the relationship between chronic fatigue and exercise.
The pilot study had established a specific and reliable set of principles which could be used as a “standard” procedure for future studies of chronic fatigue, and could fit in with the existing range of projects such as those studying the relationship between exercise and arthritis, asthma, smoking, and over weight problems etc.
He then asked me to increase the number of people in the study, and to continue it for another 12 weeks as planned, and I agreed. I then contacted the medical editor of the “News” and a second article was published which reported the success of the program and invited more people to enrol.
Essentially it said that the head of the institute reported the success of the pilot study which could be a world first, with comments by me requiring more people joining the course.
Part 3
Everything then proceeded like clockwork again without the need to make any changes at all.
At one stage I decided to contact each of the 65 people who had enquired about the course to ask them to describe, in their own words, what they thought was the cause of their fatigue. I managed to arrange 48 phone interviews in which it became apparent that it was a physical condition with many different causes, and that once you’ve got it, you’ve got it.
However, in some cases they were unable to say when it started because there wasn’t an obvious cause. In other cases it was very clear, and followed a viral infection, or a pregnancy, or a prolonged period of busy activity for months or more without sufficient rest or sleep, or an emotional incident. Some of the individuals had adapted to the problem by changing their lifestyle.
My full account of those interviews can be seen here.
When the second 12 week exercise period had passed I collected the files again and extracted and assessed the results.
By then nine people had completed 12 weeks of training, and five of those went on to complete the second, and continued to improve their aerobic capacity, although generally at a lower rate.
It was evident that they had a physical condition which initially improved with exercise, and then evened out at a lower level than normal, indicating that they had a chronic illness with a chronic limitation, and that if they exercised within their limits they could do so for as long as they wanted to.
One appeared to be heading for complete recovery, but I was unable to determine why. He may have recently became fatigued, and was at the early reversible stage, or he may have had a different ailment, and I have discussed that elsewhere.
Only two became slightly worse, and one regained the losses and returned to the previous level in the second session.
I had, at that stage, the aerobic measurements for each individual and put them in a list from highest to lowest, and then phoned the instructor and asked him to tell me who was leading the group on the running track, and who was coming last. The outcome was that the person with the highest measurable aerobic capacity was coming first, the second highest was coming 2nd, etc, and the lowest was coming last, in exact order.
In other words there was scientifically measurable data from the laboratory which explained why some people had a lower capacity for exercise on the oval.
I then arranged for another meeting with Tony Sedgewick, and told him about the findings, and he asked me to organise a larger study of 200 people for the purposes of having more influence of world opinion relating to the topic.
However, I had other problems with my health which made it difficult to do the first study, and more difficult the second time, so it wasn’t sensible or practical for me to attempt a task of that size, so I told him that I would be leaving the project to find something else to do.
I also said that the existing individuals could continue to train under the same instructor for as long as they wanted to, and he could get more longer term data from them, and that he might be able to find someone else to organise the larger study by using the same principles.
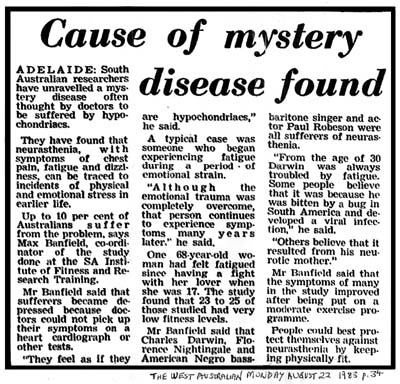
I then completed a research paper on the methods and results, and sent it to the Australian Medical Journal who sent a standard reply indicating that it was not accepted at that time, and wishing me luck getting it published elsewhere. I then sent it to the New Guinea Medical Journal, and received a reply from the editor who expressed his appreciation for the article, and commented on it’s value, but that, regrettably, it was not written in the style suitable for his journal.
I knew the value of the idea, and that if I didn’t get something published that another person could repeat the process, and get the concept published, and claim it to be their own idea. I therefore tried to get something in the news papers, so I attempted to find a freelance journalist, and was directed to someone in Melbourne who I contacted by phone. He checked the facts with the head of the institute, and then prepared an article.
From what I understand they then send it to major Australian and overseas newspapers, and get a fee for each one which publishes it.
I checked the papers in my local newsagent and found that one was published in the Sydney Morning Herald, another in the Queensland Courier, and a third in the “West Australian”. Each news editor gave the same article a different title, and the title in the West Australian was . . . “Cause of mystery disease found”. I presumed that there were more in the London, New York, and other national capital city newspapers etc, but I could not confirm it.
I then put my research paper in my filing cabinet where it had been for more than 30 years.
|
Project statistics 8 people were involved at the administrative level of the project including the head of the institute, myself, 2 research cardiologists, a general practitioner, a psychiatrist, and an instructor, and a medical editor from the “News” attended one of the meetings, and wrote articles prior to commencement, and after each successful 12 week program had been completed. 65 people made enquiries and about 25 had their aerobic capacity tested, 9 completed 12 weeks training, and 5 completed 24 weeks or more. In the first 12 weeks 6 improved, 1 remained the same, and 2 became slightly worse. Of the 6 people who improved in the first 12 weeks, all six improved slightly or significantly more in the second period, and one appeared to be returning to normal health levels. One of the participants who became worse had taken 4 weeks off during the period due to another illness, and did not continue into the next session. The other one continued and improved back to the original level. See the graph summary here. 4 articles about the project were published in the “News” between August 1982 and November 1983, and a freelance journalist from Melbourne prepared a summary which was published in at least 3 interstate newspapers including The Sydney Morning Herald, The West Australian, and a Queensland newspaper called The Courier Mail between 20th and 22nd August 1983. Project objectives achievements When Tony Sedgewick told me that his 2 researchers were busy on other projects, he asked me to organise it myself, and explained that I could do it by establishing a research team which met all of the official government requirement that a person such as myself couldn’t fulfil alone. He said that he would be part of it, and could recruit the 2 research staff, and an instructor, and that I would then only need to recruit two additional medically qualified members. I therefore interviewed several doctors. The first one to agree was a general practitioner, and the second one was a psychiatrist. I didn’t try to find a psychiatrist because the aims of the study were to find the physical basis, and a physical treatment method, but I accepted his offer because it saved some time recruiting someone else. When we had one of our first meetings he suggested we include a questionnaire to determine the possible involvement of psychological problems, and I didn’t think it was relevant to my objectives, and thought that it would be more suitable for a completely separate and different study, but as he was involved I returned his favor, and agreed to use it. The project then proceeded to the pilot study stage of 12 weeks training, and then to the confirmation stage of another 12 weeks before I decided to leave. I had then achieved three objectives . . . 1. It was the world’s first study to show that the condition involved a chronic reduced capacity for physical exertion. 2. I had verified that my exercise guidelines etc. were the world’s first safe and reliable methods, and could be used in any future research and treatment of the condition. 3. I had shown that some of the patients would stay the same, others could improve their physical capacity slightly, or moderately, and some could proceed to return to normal levels of fitness and health. However, because of the psychological questionnaires there were several issues that evolved, and I will discuss two in particular. The first was that my original aim was to help the millions of patients who wanted their condition to be recognised as real, and physical, and when some of them read my research paper they would see the psychiatric questionnaire, and think that it was my idea, and be hostile toward me for including it. The second occurred when I spoke to newspaper journalist and described the physical aspects and exercise methods, and some of their articles would place more emphasis on the psychological aspects and examples. Nevertheless, I achieved my objectives, and it is my guidelines, and principles which are now being most commonly used and discussed all around the world today, thirty years later, in journals, books, and support groups and research projects, clinics, and specialised hospitals. Somehow or other some people have been reading about my ideas and methods, and have tested them and found them to be accurate and useful, and copied them, had them published in official journals, and are claiming them to be their own, and the principles have entered the general literature, without anyone knowing that I produced them. However, I established the facts, and those are the facts. |
See here
See a YouTube video which explains the PACE trials, and how encouraging people to improve in a consistently regular manner is not the way to do the exercises properly here.
Part 4
A few years later I was listening to the radio when I heard a report about a brand new disease of modern civilisation called the Chronic Fatigue Syndrome. It was obvious to me that “new” diseases don’t suddenly come from nowhere, and that in fact it was just another label for the fatigue that I had been studying. There have been more than 100 different labels for that ailment, but I had known it as Da Costa’s syndrome, and had been looking at the research literature under the name of “neurocirculatory asthenia”.
Part 5
A few more years went by when, after a blood test, a CAT scan, a bone marrow biopsy, and a surgical biopsy I was diagnosed and confirmed as having a form of cancer called Non-Hodgkin’s Lymphoma. The cancer was evident in my blood, my bone marrow, and in every part of my body including my chest and abdomen, so I was given two months to live with no hope of a cure, and was advised to write my will. See here.
I didn’t think that I could cure cancer within that time so I didn’t even try, but just read the basic literature on the topic and left all treatment up to my doctors.
In the meantime I had just written a small pamphlet about health and decided to continue. The process of writing had been causing me a lot of abdominal pain for many years, for reasons which I had assessed as being due to postural pressure on my abdomen.
However, despite my attempts to adjust my posture I had not been able to prevent the problem, so I was usually in pain after only a few minutes. I decided to continue publishing and distributing that book regardless, until I died.
There was always the risk that writing in so much pain would cause more permanent damage to my health, but it wouldn’t matter because I would soon be dead from cancer anyway.
The pain reduced me to writing one sentence, or one paragraph, or one diagram at a time, with the occasional essay, so the book is more of a collection of facts and evidence and clues to assist me, and anyone else to understand and find the causes of many illnesses.
In the process, I did, on more than one occasion, notice notice permanent changes in my digestive function.
My objective was to describe the cause of health problems in great detail to help other people prevent such problems in the future.
In 1997 I started noticing a tightening sensation in the centre of my chest which would occur after a short distance of walking. it required me to stop and within a minute or two the pain would pass, so I started walking again. Consequently I would stop and start 5 times if I walked 500 yards. I didn’t know the cause at first, but after a few months the pain was becoming progressively more frequent until it was happening every 10 yards, so I consulted my doctor. He diagnosed it as angina and prescribed me with a drug called Noten to treat it. The pain reduced by about 90% so I kept taking it. The pain was caused by a form of heart disease and is called angina. It is due to the build up of cholesterol in the blood vessels of the heart until they become so blocked that their is insufficient blood passing through to the heart muscle. A cardiologist then advised me to have coronary bypass surgery, but I had a book about Nathan Pritikin’s dietary treatment which I read and then decided to try that method. By eliminating cholesterol from my diet the build up in my arteries stopped and began to reverse, and after about 6 months I could reduce the dose of the Noten to half, and then none, and the pain didn’t return, so I was cured. However, it probably took about 2 years before I had fully recovered. See my full report here and my audio CD on the topic here.
Another year passed and I had learnt to type, and I had began experimenting with my writing position to prevent the abdominal pain. At first I put a 6 inch high shelf on my desk and noticed that I had less pain, and a few months later built another 6 inch shelf on top of it, and the pain became less of a problem. I also started to stand at a platform and write, and adding an angled platform which was somewhat like an artists stand, or a music stand with an angled attachment for the music sheets. I then learned to use a computer, and later, when I put the keyboard at waist height, and the computer screen at eye height I could type without having to lean forward, and the abdominal pain virtually stopped altogether. I have had some minor problems since, but nothing like the repetitive, and often long lasting and severe pain that I had previously experienced. See here.
While I was writing the book I was describing undetectable illness and pain which had been referred to in the following manner in the past . . . “It doesn’t show up on x-rays or blood tests therefore it is all in the mind”.
My intention was to describe the causes, aggravating factors, and nature of those pains in so much detail that it would be obvious to everyone that they were real physical conditions. The only difference was that they didn’t show up on x-rays like the illnesses which were called “physical”.
At around about that time a small lump about the size of half a golf ball had appeared on my neck, and over a period of 18 months had grown to the size of a hens egg. The cancer had turned aggressive so I had surgery to remove the lump, followed by six months of CHOP chemotherapy. Another 19 months went by when a scheduled CAT scan revealed that a cancer the size of a large orange was blocking my left kidney. I then had surgery to remove most of it, followed by three months of DHAP chemotherapy, and after making a partial recovery from that I went into hospital again to have a stem cell transplant, followed by MabThera chemotherapy.
I then had four years of side-effects which I have described here. and made a complete recovery except for baldness.
Part 6
Another year or two went by when a friend of mine suggested that I add some of my ideas to a new online encyclopedia called Wikipedia.
However, I had been publishing my own books and website since 1994 so I hadn’t needed newspapers or journals since then, and my website had often been in the top ten list on the Google search engine for Posture, and I didn’t even notice Wikpedia mentioned anywhere even if it was there, which I doubt.
My friends also told me that school teachers and university professors would not allow their students to use it as a reference because it had been compiled by teenagers, vandals, and amateurs, and was poor quality and unreliable
Nevertheless when another friend told me about it I decided to have a look.
It said that you could write about anything, including your own research, because they preferred reviews from other people. Consequently, if you did, some of the other editors might delete it on the grounds of conflict of interest etc. so I decided not to bother.
However, when it was again recommended to me I decided to join and add about a paragraph of information per week, on any one of 100 miscellaneous topics, particularly from history, because it wasn’t known to most modern writers, and I would be improving it’s knowledge base, without even trying.
I had been writing in a more or less anonymous way for 30 years to avoid prejudice and discrimination, and I did that by using my real name of M.A.Banfield instead of Max Banfield, and I never showed a photo of my face in my essays, books, or website.
In that regard, when Wikipedia allowed people to edit under their real name, or by using an ID, I chose the ID method.
I had been writing about posture and health for much of the time so I called myself “Posturewriter”.
I then proceeded to add information to several pages. For example, on the page about chest pains I said that poor posture was a cause, and on the page about Varicose veins I added tight leg garters as a cause.
I then received an email from someone who I had never met, and who had read my book in her local library and told me how useful it had been to her in understanding her own illness, and how much she appreciated it.
I therefore asked her if she would write an independent review for Wikipedia, and I said that my 1000 page book was complicated, and that I would prepare an accurate one page summary for her to rewrite in her own words if she agreed with it.
She was an excellent writer and provided a better article than I could have produced myself, but a some time passed when I made a few minor changes and asked her to add the word “hypochondria”
It changed the page from being about “posture” as a cause of “multiple undetectable aches and pains” to a page about “posture” and “hypochondria”.
Within a short time an editor set up a discussion to have the whole page deleted, and up to six completed it with the comments “delete, delete, speedy delete” etc.
It was obvious to me that there was a group of editors who didn’t want anyone to prove that the psychology theories were wrong, or even shed any doubt on them. They wanted all of the readers of Wikipedia to believe that if an illness didn’t show up on x-rays that it must be “all in the mind” because no other explanation was known or possible.
They accused the woman of breeching my copyright, so I entered the discussion to say that I had given her permission to write the review, and then they required me to prove that I was the author, in which case I had to give my real name, and the name and dates of publications. Despite giving them all of that information they deleted it anyway, without giving a reason, and although I had the opportunity to appeal the decision, I gained the distinct impression that it would be a waste of time, so I didn’t bother.
Part 7
I then started looking for other pages to add to such as posture, backaches, faintness, corsets, fatigue, rickets and fashion and health etc, when I came to a page called Da Costa’s syndrome.
It had only four lines of text, and no references at all, and an invitation to help improve it, so I started by improving the details in the description, and by adding some top quality references, such as the original research paper by Jacob Mendes Da Costa from 1971 who the ailment was named after. I then added a summary of my own ideas and research.
Within a short time two editors started criticising me in an arrogant, dictatorial manner, as if they were the owners or Wikipedia who had the authority to dish out orders and treat me like a fool. They deleted everything I wrote on the grounds that there was nothing about my ideas in what they called the “real” literature, and described me as a non-notable fringy kook who was writing nonsense. They also argued that my ideas took up too much space, so abbreviated it and put it back, and then immediately acted as if I had been deliberately disruptive, and they deleted it again, and then tried to set up three different discussions to get me blocked from the page, including one where they wrote thousands of words accusing me of “conflict of interest”.
However they said that they appreciated my other efforts on the page where I had described the ideas of other researchers.
Those references were top quality articles from the history of the research so I began adding more.
The two editors became even more hostile and accused me of using poor quality information from references which were “old”, “out-of-date”, “obsolete”, and “from before most editors were born”.
A few more months went by when two uninvolved editors suggested that the dispute could be resolved if each of us wrote and article outside of Wikipedia, making a total of three, and then put them back for them to assess and produce one article which represented a truly “independent” and “neutral point of view”.
My two critics didn’t write anything, but when I put mine back and nobody criticised it, I used it to replace the existing one. My two critics then deleted it, and replaced it with the previous one, which was theirs, and which they called “neutral point of view”.
Within a month they had managed to get an administrator to use their “ignore all rules” policy to ban me.
I had the opportunity to appeal that decision, but I had gained the impression that if the could ban me by “ignoring all the rules”, then they could keep me out by “ignoring all the rules” so I didn’t bother.
I then decided to become a critic of my 2 critics and began by gathering evidence that they were both prolific liars.
I had also noticed that while I was contributing to pages about posture and Da Costa’s syndrome, and my two critics were describing it as nonsense and deleting it, that other anonymous editors were rewording the same ideas and adding them to other topic pages.
That process continued after I was banned, so some of my ideas have appeared in pages about posture, chronic fatigue syndrome, postural orthostatic Tachycardia syndrome, orthostatic intolerance, and costochondritis, which are essentially just different labels for the same ailment.
In other words they don’t want any of their readers to know that I exist, and that I produced those ideas, but they do want the ideas because they are the best available, and the want Wikipedia to get the reputation of having the best information.
I have also noticed that they are manipulative individuals who have portrayed themselves as highly experienced, trustworthy, and respectable, rule-abiding members of the Wikipedia community, so when I criticise them they are defended by their supporters, and the other editors who feel the need to defend all of Wikipedia’s reputation.
Part 8
A few more years went by when I joined Twitter and saw a comment about a person called Simon Wessely being granted the John Maddox Prize, for his courage in science. Various websites report that he began his studies into “medically unexplainable illnesses”, and was helping patients overcome the stigma of the disease by arguing that the problems were physical and not mental, and he made specific reference to the “Chronic Fatigue Syndrome” which had previously been trivialised as just “Yuppie Flu”.
It was also reported that he had been involved in defining the condition, and developing “new” methods of treating it called and “Graded Exercise Therapy”. They also refer to his style of treatment as involving light exercise gradually improving with time by avoiding the levels which cause fatigue.
A few months later he was granted a Knighthood for his contributions to medicine, on 1st January 2013.
I have spent 37 years, since 1975, intermittently, but consistently describing in detail, and researching the physical basis for undetectable illnesses, including chronic fatigue, and I developed the exercise method for treating it in Adelaide in 1976, and scientifically proved it and had newspaper articles reporting the success between 1982-4. Simon Wessely started three years later, in London, in 1987.
Part 9
Since writing this essay, I have found some more information. Firstly, I would like you to recall that after I proved the concept of training within limits to get success with 12 week exercise programs, I then reproved the concept in a second study, which made it a reliable and standard method. The head of the research institute then asked me to do a larger study of 200 people to have a major influence on world opinion. However, I still had health problems and a study of that size was not practical so I left the program.
I then prepared a research paper summarising the results, and sent it off to two medical journals. When they didn’t publish it, I put it away in my filing cabinet. Therefore, it is quite likely that the only thing that future researchers could copy was the general principle, but not all the details, which is probably what Simon Wessely did, from 1987 onwards.
Twenty years later I joined Wikipedia and added some information about that project, but two other editors began defaming me with their ill-mannered, relentless, hostile, and vindictive insults aimed at discrediting me so that they could delete almost every word I wrote, and then they arranged for the “ignore all rules” policy to be used to ban me..
I therefore decided to look for my old research paper from 1982, and scan it into my computer and load it onto my website, so that other people could see that my ideas and research existed, and were better than the nonsense which remained in Wikipedia.
However, something else happened which I will suggest.
Firstly, the two editors or their anonymous cohorts then rewrote the ideas methods in different words, and put it on other pages, to steal my ideas.. However, other researchers could do the same, and then get the results published in medical journals, and claim it to be their own concept.
It would take awhile to decide to copy the methods, by 2009, and about a year to organise a major study, making it 2010, and then a year or two to do the major study, and submit it to journals and get it published.
A few months ago, in January 2013, I saw a report of a major study by a colleague of Simon Wessely’s, professor Peter White, who had just completed a major study of chronic fatigue and exercise, involving 650 people, and had it published in a medical journal.
In summary, I developed and scientifically proved and standardised an effective and reliable method of exercise for chronic fatigue in 1982. Simon Wessely began copying my general principles in 1987, and Peter White began copying the details of my methods after they became available on my website in 2008.
Part 10
I would now like to finish by discussing the fact that when I proved the concept in 1982, I knew that other researchers would have to use my ideas in future, because all other methods would fail. I was also aware that they should properly and ethically give me the credit, but also that some researchers would be tempted to claim the method to be their own.
My first indication came when I heard the announcement of a brand new disease called The Chronic Fatigue Syndrome a few years later, with comments that it was a physical condition of unknown cause.
I later heard occasional comments in the media about treatment methods which were virtually identical to the ones which I had proposed, and was continuing to write about in my books and website, and I got the impression that there was not just one, but several people copying me, but I didn’t investigate the possibility. I also vaguely remember hearing the name Wessely mentioned.
However, when I joined Wikipedia in 2007 I was soon being criticised by one particular editor, and their constant tag-teamer who called my ideas and research stupid nonsense and rubbish, and deleted it.
I wondered why they spent the next 12 months insulting me, and were so hellbent on getting me banned.
However, four years went by when, in about October 2012, I learnt about Simon Wessely getting the John Maddox prize for his contributions to medicine, with respect to his study of the chronic fatigue syndrome and “Graded Exercise Therapy”.
I then searched for information about that method, and found that it involved gradually improving the level of fitness by exercising regularly, by staying below the levels which caused fatigue etc., and that was one of my key principles.
I then became curious to know when he began studying this topic, and soon found that he started in 1987 in London, just four years after I scientifically proved the method in Adelaide.
I then began looking for, and providing evidence that he has copied my method, and has been reading about my observations, descriptions and ideas in my books and website etc, since. He has been shadowing me, and learning about the ailment, and how to manage the symptoms, and then getting the ideas published in books and medical journals, while claiming them to be his own ideas.
Then, in April 2013, only a few weeks ago, I became curious to know if Wikipedia had a biography page about Wessely, and if my two critics were so determined to get me, and the information about my research out of Wikipedia, so that nobody would notice, or even bother to ask the question if he copied me or not.
I found that Wikipedia has a very large page about him which thoroughly documents his numerous awards and prizes for his contributions to medicine, primarily in the area of chronic fatigue research. He has dominated most international medical discussions on the topic for thirty years.
The following words are a quote from that page .
|
“He has published most widely on aspects of chronic fatigue syndrome, including its aetiology, history, psychology, immunology, sociology, epidemiology and treatment.[1] . . . In the first years after the introduction of the diagnosis chronic fatigue syndrome the condition was often mocked in the media, for example being described as “yuppie flu” |
He has quite clearly been copying my ideas and methods and claiming them to be his own, and he is being protected by two of Wikipedia’s editors, namely WhatamIdoing and Gordonofcartoon, who have defamed and discredited me and my research, and made certain that the public don’t know that I exist in that internet publication which now dominated the world.
I will end my talk now with the suggestion that they are treating you like mushrooms by keeping you in the dark about me, and feeding you on bullshit.
I want you to reverse the process and drown them in their own bullshit;
You can do something about the plotting and scheming of Simon Wessely, and the two Wikipedia editors, by telling every man, woman, and dog on the planet, and especially in their own home suburbes, that I did it first.
Get the two editors banned from Wikipedia, and Simon Wessely stripped of his prizes and knighthood.
Thankyou for listening. I will now answer any questions if you have any.
A quick summary of my ideas about Chronic fatigue syndrome and how they have been copied
When I was a teenager I had a lot of experience in sport, gymnastics and swimming.
However, by the age 25 I had various health problems including exhaustion which had accrued for various other reasons, and were not responding to any form of medical treatment so I decided to try to solve those problems myself.
Naturally, as you would expect, one of my first attempts was to join an exercise program with the idea of starting slowly and gradually improving my level of physical fitness until I returned to normal health.
However, I was unable to keep up with the other people in the course, so rather than stopping the training I decided to slow down and keep going. I could only do the light exercises, and walking, and slow and intermittent jogging.
I was very keen to get back to normal health, so naturally, I would try to increase the level of exercise each week, but when I did that my heart rate would increase abnormally, and I would have problems with my breathing, so I decided to slow down again, and keep on training, and increasing in a much more gradually way.
My fitness did improve, but then reached a level at which it remained the same regardless of the fact that I was doing more exercise, slightly faster, and more often per week, so I concluded that I had a physical limitation, and could remain relatively free of symptoms if I stayed within it.
I also drew the conclusion that the fatigue whIch I was experiencing at other times was due to similar factors related to the same physical limitations, and so, after making some very detailed observations about general lifestyle I decided to do less hurrying etc, and reduce the number of activities during the day, and their duration, and to get more rest in between etc.
By using those methods for a few years my health very gradually stabilised, and I became less easily fatigued.
I also wrote about such things in great detail, and in plain English, and had my ideas published as widely as possible so that doctors and patients would have a better understanding of the problem, and be able to treat it more effectively than before.
In 1982, when I discussed those ideas with Tony Sedgewick, the person in charge of the South Australian Institute for Research and Training, he asked me to co-ordinate a research project, where I was able to scientifically prove those principles.
About 3 years later I heard news reports on radio and TV about a brand new disease called the chronic fatigue syndrome, and I knew immediately that it was not “new”, but was just another label for the type of fatigue which I had been studying.
Many more years went by, when, in 2012, I found out that a person by the name of Simon Wessely had been given the John Maddox Prize, for his work in defining the chronic fatigue syndrome, and treating it with a “new” method called “Graded Exercise Therapy“, and “Cognitive Behavioural Therapy“. Soon after that he was knighted for his contributions to medicine.
When I searched for descriptions of those procedures, I found that the method of exercise involved improving gradually, and avoiding the levels which cause fatigue, which is the same principle which I developed. I then found that the Cognitive Behaviour Therapy was basically the same principles which I developed for adjusting lifestyle and related factors.
I then found various reports which said that Simon Wessely began his study of chronic fatigue in England, in 1987, just three years after I completed and proved my research at the IFRT in South Autralia.
See a YouTube video of a debate about these issued in the U.K. parliament on 6th February 2013 here.
See website reporting the criticisms and comments about the failure of the 2012 PACE trials here.
|
A comment of the criticism of the method I Invented the method of exercising to treat my own chronic fatigue in 1976 and gained improvement which was better than dozens of pills which had been prescribed by my doctor, and which were ineffective and had harmful side effects. I published my ideas to help other patients by providing information on how I did it. Some patients will not be healthy enough to do what is required so they should not even try to start. However many CFS patients can walk about the house, and walk to and from shops etc. There is absolutely no reasons why they can’t start at that level of exercise because they can already do it anyway. The only difference is that they are doing it regularly in a group twice per week. They can then try to improve their level of activity at a very gradual rate, and according to how they feel, not according to what anyone else says they should be able to do. The method was never meant to be compulsory, and no-one was ever forced to do it. It was designed to be an additional treatment to be considered where all other methods failed, and those who don’t want to try it don’t have to. The criticism of the method is based on the misunderstanding that people “must” do it, or that the people trained too hard and had harmful consequences. However, that was never a part of my method, and didn’t happen in my case, or in the project that I organised in 1982. |
The Chronic fatigue exercise program design change
I developed a method of using exercise to treat my own chronic fatigue in 1976, and seven years later was invited to design a project for the South Australian Institute For Fitness Research and Training for other people with chronic fatigue. It was successful, and the principles which I defined have been used in research programs ever since. See here and here.
There is no difference between my method in 1982 “exercise within your limits” , and Simon Wessely later saying “stay within levels which don’t cause fatigue“, and the modern 2013 encyclopedia which says ‘stay within your energy envelope‘ .
In 1975 when I developed the idea of staying within my own exercise limits, I also applied the same principles to my daily activities and lifestyle to gain a better control of my health in other situations.
A description of that method which is given without any mention of my name can be seen in Wikipedia here. Another description can be seen where it is referred to as The energy Envelope Theory here.
Ordinary exercise programs and those which failed
People join ordinary fitness classes for many different reasons. For example, they may just want to get fit, or they may be preparing for the next sporting season, or a fun run. Some may also be using exercise as a way of recovering from an illness or injury.
In some cases they will be given a medical test to determine their aerobic capacity at the start, and again at the end of 12 weeks to determine their level of improvement.
The general idea is to start exercising at mild levels with slow walking or jogging, and to increase the number and speed of exercises each week. Usually some people will drop out in the first week, or the second etc, but some will still be there until the end.
However, when researchers were trying to determine the effects of regular exercise on patients who had chronic fatigue they found that all of them dropped out of the course before finishing, so there were none left to test.
One such program stated that the patients could not or would not do the prescribed exercises.
Identifying the problem
When I saw those comments I knew what the problem was and decided to solve it.
I assumed that the patients had physical limitations of varying degrees from person to person, and that as each individual exceeded their personal limits they would get distressing symptoms and drop out of the course.
Consequently some would drop out on the first day, others in the first week or month, and none would be able to keep up with healthy people until the end.
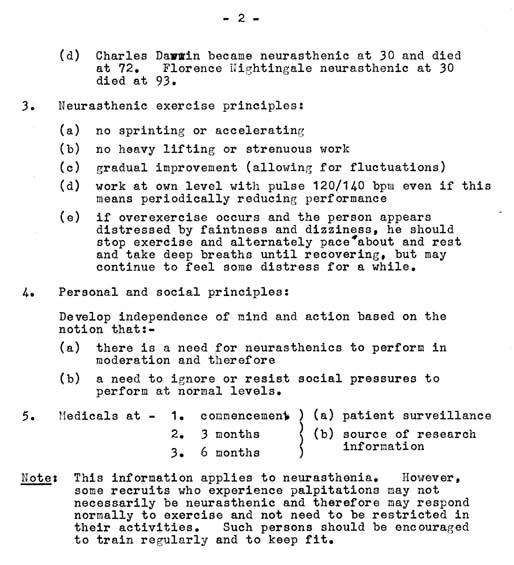
The exercise principles from the 1982 IFRT project
The exercise program which solved the problem
Therefore I recommended that chronic fatigue patients be kept in a group of their own, and that they be given instructions to exercise at their own level, within their own limits, and improve at their own rate. if they exceeded their limits to the extent that their symptoms began to trouble them then they should slow down, and rest or stop, and then continue at a more moderate rate, or perhaps start again the next week at a lower level. They were also able to leave the course at any time they wanted if necessary.
Consequently some of them were able to continue exercising on a regular and consistent basis for 12 weeks, and it was possible to gain scientific data on their aerobic capacity, and some did gain measurable improvements.
In fact, the program was so successful that it proceeded into a second period, and then a third, while I was still organising it, and it continued after I left. See some newspaper articles which record the success of my research project here, and online here and about my research here and here.
(Note that some people with chronic fatigue might not be able to exercise, so nobody was forced to join the classes, but they were invited to if they thought it might be helpful).
Why other researchers have copied my method and are now using it and calling it the best
Up until 1975 there had been many attempts to get chronic fatigue patients to exercise but there was a large element of guesswork by doctors, and a considerable element of doubt about the process in patients, and mixed results.
In 1975 I developed a method of treating my own chronic fatigue by using the trial and error approach, and in 1982, when I was invited to design the research project for other people, I removed the element of doubt.
Since then doctors have been able to organise such programs with confidence, and patients have been able to see the logic and sense in setting their own limits, and have been able to participate with confidence.
You can now appreciate why it would be impossible for anyone to get results unless they used my method, which is why it has been copied since by many organisations around the world, including Simon Wessely. It as been called PACING and Graded Exercise Therapy, with slight variations on the theme, but where the basic principle which I developed, are the same.
See my report on other people who have copied the idea here.
This is description of Graded Exercise Therapy by the Mayo Clinic . . . “The graded exercise therapy means exercise using a physical therapist to set up a program to gradually increase the intensity of the exercise so as not to fatigue the individual.” (end of quote) here. That quote is just a rewording of the principle which I told the instructor to use at the IFRT in Adelaide in1982 here.
The standard method of gaining Scientific proof of concept
including the Peer Review Process
Step 1. You need to produce and idea for solving a problem – which I did
The method had three principles
. . . (a) The person with chronic fatigue needs to exercise at their own pace and within their own limits to make gradual improvement where possible.
. . . (b)The person needs to needs to modify their general lifestyle in a similar way.
. . . (c) The person needs to be given instructions on the general nature of the problem and how to modify their lifestyle, and other factors which may be contributing to it.
Step 2. You need to establish a project to test and prove the concept – which I did.
Step 3. You need to redo the procedure to prove that the first results were not just a coincidence – which I did.
Stop 4. You need to redo it again to confirm the results – which I did.
Step 5. The same methods need to be retested by people who are independent of the original person, and is generally referred to as the peer review process. The same methods which I perfected between 1976 and 1983 have been used in many studies since, and again recently in January/February 2012 by professor Peter White, as can be seen in the table below . . .
|
“Peter White, Professor of Psychological Medicine at Barts and the London School of Medicine and Dentistry, part of Queen Mary, was the lead co-principal investigator of the PACE trial and co-author of the latest paper.” A quote about his results from another website can be seen below . . . “CFS is a long-term and debilitating condition that affects around 250,000 people in the UK. Symptoms include profound physical and mental fatigue (characteristically made worse by exertion), muscle and joint pain, disturbed sleep and both concentration and memory problems. The researchers studied 640 participants with CFS who were randomised into one of four treatment groups: Specialist medical care (SMC) alone; The findings showed that those who received CBT or GET, in addition to SMC, were three times more likely to meet the criteria for recovery than those receiving SMC alone or in combination with APT. Overall 22 per cent of those who received either CBT or GET, in addition to SMC, met the criteria for recovery, compared to eight per cent after APT in addition to SMC, and seven per cent after SMC alone. There were similar patterns of recovery however CFS was defined, including those who were diagnosed as having myalgic encephalomyelitis (ME), thought by some to be the same as CFS and by others as being different.” (end of quote) See here. |
One fact remains – nobody is acknowledging that I produced the original concept which has given 2 Wikipedia editors the opportunity to argue that my research was “NON-NOTABLE”, and “ORIGINAL RESEARCH” which has NOT BEEN INDEPENDENTLY VERIFIED and therefore had to be deleted. See here.
The 2011 NIH workshop drew exactly the same conclusions about treatment which I defined in 1982
Also notice that the report from the NIH 2011 workshop contains the following treatment recommendations which were defined in my research project in 1982. One page from my project can be seen above, and the other relevant pages can be seen here.
Since then I have described how I manage the daily symptoms in great detail in essays, books and on my website, and many people have copied them, and most people who use those ideas don’t know who produced them because they have found the methods in books written by people who copied me without acknowledging the source.
|
This is what the NIH (National Institutes of Health U.S.) report concluded almost 30 years later. It was called The State of Knowledge Workshop, and was sponsored by The Office of Research on Women’s Health, the National Institutes of Health, and the U.S. Department of Health and Human Services in collaboration with the Trans-NIH ME/CFS Research Working Group . I quote . . . “Pacing, to avoid over-exertion and collapse I have been reporting how I manage these problems in my own life for thirty years, and yet this conference concludes that it would be a good idea in the future? I knew that it was a good idea soon after I started reading medical books because it was obvious that doctors didn’t understand the problem and that they never would until someone like me explained it all. |
The medical advice given to chronic fatigue patients in 1975, and why I had to develop something new
The general advice which doctors gave to all chronic fatigue patients, including myself, in 1975, was that there was no evidence of disease on blood tests and x-rays, and that therefore there was nothing physically wrong, that the fatigue was normal, or due to laziness, the fear of exercise, and the lack of exercise, so just think positive and ignore the symptoms and run faster, and faster, and faster until you are healthy again.
I knew from personal experience that the advice was wrong, and that I would have to develop my own methods of treating the ailment. e.g. See here. Nowadays most chronic fatigue patients are treated with my methods which include exercising within limits, and leading a lifestyle within limits, and everything related to that general idea of reducing and modifying activity levels to an appropriate and manageable level..
The S.A. Research Matched Russian Results
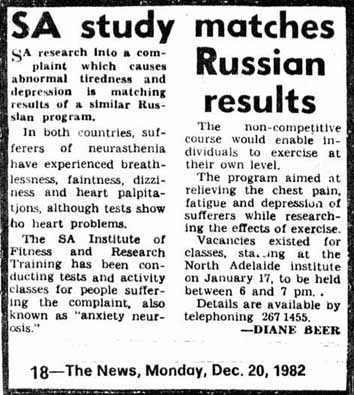
One of many newspaper articles which reported the success of the program in 1982.
Nowadays patients who have persistent problems with fatigue are sometimes diagnosed with the chronic fatigue syndrome, but in 1980, in the U.S. it was still being called neurocirculatory asthenia, and in Russia it was called neurocirculatory dystony where V.S.Volkov measured the aerobic or fitness capacity and found it to be lower than normal. Other researchers were trying to determine if regular exercise would improve the fitness and health of such patients but were not able to because the patients were dropping out of their programs before the effect could be re-measured.
Meanwhile, back in South Australia in 1975, I had that ailment and thought that regular exercise might improve my health so, in 1976 I joined a course at a fitness research institute. I was unable to keep up the pace of the healthy people, so rather than drop out, I decided to continue at a lower pace of walking and slow jogging. Everyone in that course had their fitness measured at the start and after each 12 week session, and mine improved but then stabilised, but was still below normal. After about ten months I injured my knee cartilage and had to stop.
I also started reading the medical literature and when I found out about Volkov, and the problems that other researchers were having, I knew that I could solve them. I was later introduced to the head of the research institute, Tony Sedgwick, in 1982, and I explained the problem and the solution. He immediately recognised the potential and ultimately invited me to design an exercise program specifically for chronic fatigue patients. I also explained that some of the patients might not be able to participate, but that some would, and the project proceeded according to plans with success and results as predicted.
I knew that those exercise principles would be the template for all chronic fatigue and exercise research in the future, and it is evident in subsequent programs called PACING and Graded Exercise Therapy.
Note that many attempts have been made in the past to encourage chronic fatigue patients to train at the same pace as healthy people, but they have invariably failed. The only effective way to get such patients to exercise is with mild but consistent activity.
However, some critics of that method argue that it isn’t enough exercise???, or isn’t real exercise???, and therefore won’t be any use???. They are essentially arguing that a person must run fast enough to build up a sweat before any benefits can be gained.
However, that simply isn’t true, and the idea of getting patients to exercise at higher levels is impractical. See why here.
I have studied this topic more extensively than any of my critics.
Another example of the independent use of my research by Fibromyalgiaaustralia
An organisation called Fibromyalgiaaustralia. has a four page account of the nature and treatment of chronic pain and fatigue for July 2012. The following table contains quotes from some of the comments.
|
“Fibromyalgiaaustralia education, best practice, empowerment & management Strategies for Managing Chronic Pain July 2012 National Pain Week” “Exercise, Posture, and Movement FM patients especially can help reduce their pain by experimenting with how to hold their body and how they move. Exercise is one of the most commonly prescribed treatments for FM and can be helpful for CFS as well” . . . and . . . “Pacing – A frequent cause of pain is overdoing or having an activity level that is beyond a person’s limits. Pacing offers a way to bring stability and control by keeping activity level within the limit imposed by illness. Pacing can involve a variety of strategies including . . . Reducing overall activity level Setting priorities and delegating Taking scheduled rests Having short activity periods Switching between high and low intensity tasks Using the best hours of day for the most demanding activities Knowing mental and social limits Keeping records to see links between activity and symptoms” (end of quote) On the fourth page they have a section called Problem Solving which states as follows . . . “You can gain some control over pain by identifying the situations that trigger or intensify pain and then taking steps to change them ” (end of quotes). See my thorough and detailed research into the relationship between posture, fatigue and pain here and my eBook here. See my thorough and detailed research into chronic fatigue and exercise here. |
From the International Encyclopedia of Rehabilitation 2013
Benefits from graded exercise first demonstrated in a 12 week study by Fulcher and White in 1997???
See my report on the typical treatment of chronic fatigue before I wrote my theories between 1976 and 1982 here
She how I developed my theories of physical cause here.
|
The following description is about another article by other authors and has references between 1997 and 2012, but most of that article is a direct or indirect copy of my observations, descriptions, theories, and research which started in 1975 and has been presented in essays, books, journals, newspapers, and my website up until the current time. |
This is a quote from a current website of 2013 called the international Encyclopedia aof Rehabilitation . . .
“those people with ME/CFS who are able to stay within ‘energy envelope’ show significant improvements (Jason et al. 2009)” . . .
“Pacing self-management aims at stabilizing the patient’s health status. After the initial stabilization phase, a grading phase is initiated and comprises of graded activity or graded exercise therapy (Figure 1). During the grading phase, the same pacing principles are applied to grade both daily activities as well as exercise levels. When determining an appropriate exercise level, a formal, regulated exercise regime that is gentle, graded, flexible and manageable according to each individual’s capabilities is required. Support for this type of ‘grading’ for people with ME/CFS comes from an observational study (Coutts et al, 2001) and a well-designed randomized controlled clinical trial, which reported that paced and individually-tailored graded exercise was superior to relaxation and flexibility training in patients with ME/CFS (Wallman et al. 2004). The use of graded exercise therapy for people with ME/CFS will be further discussed below (section 4.5) . . .
“Benefits associated with graded exercise were first demonstrated in a 12-week randomized, controlled trial by Fulcher and White (1997) that compared the efficacy of graded exercise to flexibility exercises in ME/CFS participants. Since then, a number of studies have examined the effectiveness of graded exercise therapy for ME/CFS (e.g. Weardon et al. 1998, Powell et al. 2001). According to the Cochrane Library, graded exercise therapy is effective in the short term for treating ME/CFS patients (Edmonds et al. 2004). However, it should be acknowledged that graded exercise therapy is not suitable per se for all people with ME/CFS at any stage of their illness. Rather, graded exercise therapy can be one component of an overall rehabilitation approach to ME/CFS . . .
Introduction of exercise that is beyond a participant’s capacity may not only promote a relapse, but can also result in feelings of demoralization and pain, thus reinforcing avoidance behavior (Figure 1). Therefore, Wallman et al. (2004) introduced the pacing approach into graded exercise therapy for people with ME/CFS. They designed a graded exercise program that is flexible, realistic and manageable according to each individual’s needs and abilities. The program schedules rest periods in conjunction with the exercise periods, as this can help in establishing a manageable routine that can assist in promoting a sense of control over one’s life (Pheby 1997, Sharpe et al. 1997) . . . “Cognitive behavioral programs for people with ME/CFS combine a variety of treatment options, some of which are explained above (e.g. education, time-contingent activity management, time-contingent graded exercise therapy, stress management, sleep advice, goal setting, etc.) . . .
When explaining to people with ME/CFS that rehabilitation is not a cure for ME/CFS, it should be explained that conservative strategies will address perpetuating factors of ME/CFS, and hence lead to increased functioning rather than full recovery.” (end of quote) See here
The majority of the information in that article, about the physical aspects of CFS, could have been copied from the detailed descriptions in my essays, books, website, and research. e.g. See here. They may have been copied by earlier authors, so that since then the later authors were not aware that the ideas came from me, but nonetheless they are my theories and methods.
However, the authors mention the concept of kinesiophobia (the irrational fear of movement), and exercise phobia, which is a separate issue, and is not the cause of the abnormal response to exercise. They also refer to the “catastrophizing thoughts”, and “hypervigilance of symptoms”, and “somatization”, which refer to imaginary, exaggerated or psychological causes.
I have said many times before that the symptoms of chronic fatigue are completely different condition to the “fear” of exercise etc, and that those aspects are common to all illness, not just CFS. See also here and here.
I have also explained that the breathing abnormality in CFS is due to some sort of physical problem and has nothing to do with panic induced hyperventilation. See my YouTube video here.
This is some of what that other author says . . .
“decreased lung function (De Lorenzo et al. 1996) . . . a decreased peak oxygen uptake during exercise performance testing (De Becker et al. 2000), and an increased prevalence of hyperventilation (59%) compared to healthy controls (22%) (Bazelmans et al. 1997). Hyperventilation in not a causal factor for ME/CFS, but is likely to be a perpetuating factor for some patients, especially those having difficulties with acceptance (Bogaerts et al. 2007). See here.
What the people who copy my ideas don’t know
When I began studying this topic in 1975, I soon found, within a few years, that other people hadn’t previously understood the problem, so I started describing the symptoms in detail. However, I knew that some individuals would recognise the value of the ideas, and that I hadn’t been able to publish them in medical journals, so they would reword the concepts and get them published and claim them to be their own. I therefore decided that I would not publish everything, or even talk about some of the important principles which I developed.
When I read the encyclopedia entry above it is obvious that the authors have read my publications and copied them, or have read the work of other copiers, and not known that I was the originator of the ideas. At a rough estimate I would say that they have copied at least 20 of my concepts in a very clear, orderly, and articulate way, but they come from my books and web site where they are randomly scattered about in places where I thought of each of them one at a time, sometimes years or decades apart.
However, they have not published my unwritten ideas, because they haven’t got anything to copy, and they haven’t mentioned anything related to them, because they haven’t developed the ideas themselves.
In order to prevent anyone from copying more details etc. I will give a quick summary.
l,klo
I then empirically, and later scientifically proved that it was a physical problem, and not a mental one, and that patients could be given instructions on how to exercise, and in some cases gain improvements, but not necessarily a cure for their ailment.
The encyclopedia above gives the general impression that it is a physical problem, with physical limitations, which they refer to as the “energy envelope”, and the treatment is “graded exercise therapy” and “education“.
Some of my unpublished ideas, which are impossible to copy, are the Gh calculation, the Significant L principle, and the CB method etc.
How and why Simon Wessely has copied my research
My previous publications and newspaper reports about my research can be seen here.
It appears as though Simon Wessely has been regularly reading my essays, books, and website, and stealing and rewording my detailed observations, descriptions, ideas, and methods, and then getting them publshed and claiming them to be his own, and building a very successful research career for himself. He has recently been awarded the John Maddox Prize for courage in science, and been knighted for his contributions to medicine.
He has stolen my evidence of a physical causes for undetectable illnesses, but at the same time, has never mentioned my book as the source, and he has taken the credit in some places, but in others he is talking about the effect of illness as if it is just “beliefs” or “attitudes” rather than facts. See here.
There is the general “image” that all doctors are wise and all patients are “stupid” so the fact that I solved most of these problems upsets that false impression.
The following chart shows what I did, and what Simon Wessely has copied.
|
In 1975 I was told that there was no evidence of illness on blood tests or x-rays and that there was nothing physically wrong with me so I became interested in undetectable illnesses which were called hypochondria. I determined that one major physical cause was posture, and wrote The Posture Theory. See here.. Another major cause in the 19th century was tight corsets which crushed, deformed, and displaced the internal organs. See my book published at the rate of 150 pages per year between 1994 and 2000 here The subtitle of the current book is “The Physical basis for Undetectable Illness“. |
Simon Wessely is a psychiatrist who is described as becoming interested in “medically unexplained illness” and chronic fatigue in 1987. He says that he was trying to help CFS patients by saying that their symptoms were real and not imaginary as had been previously claimed. (The psychiatric profession started those ideas). e.g. See here His wording relates to “Medically Unexplained Physical Symptoms) which is abbreviated as MUPS. It is just modern jargon for hypochondria, as is “Somatoform Autonomic Dysfunction”. |
|
One of the symptoms was chronic fatigue so I studied it for four years before writing a theory of physical cause and developed methods of treating the symptoms which included 1. exercising regularly within each persons physical limits 2. leading a modified and less demanding lifestyle than normal. e.g. instead of doing 10 things a day, do 5, and instead of hurrying, be casual in doing things. I then designed a program of exercise for the South Australian Institute for Fitness Research and Training in 1982 where I was able to scientifically prove that it was a physical condition. See here |
Wessely is reported as developing the “new” methods of treating chronic fatigue syndrome called “Graded Exercise Therapy” and “Cognitive Behavioural Therapy“, which have been described as the best and most effective methods available today. |
|
While I was studying those aspects I became aware that chronic fatigue in civil life had the same symptoms as Battle Fatigue in war time, so I began studying that literature, and later joined Wikipedia where I wrote the history of the ailments in the page called Da Costa’s syndrome. See here, and on my website here. |
Wessely became interested in the Gulf War Sydrome and started developing methods of treating soldiers and veterans with similar ailments. e.g. See here |
|
The Wikipedia article about The Posture Theory was deleted, and then two editors started criticising and deleting all information about my chronic fatigue and exercise research. They also deleted almost every factual and accurate statement I made on the Da Costa’s syndrome page,and started a relentless smear campaign to get me banned. They argued that the topic was not important and that all of my contributions were worthless, non-notable nonsense and crap. See an example of the insults here, and more here and how they defamed my character here The deletion of information about my CFS/exercise research |
In 2012 Wessely was given the John Maddox Prize for his courage in science and for persisting despite death threats from chronic fatigue patients for the things he said about them. He was also Knighted for his contributions to medicine in relation to th mental health of war veterans, but that mainly relates to the fatigue which affects some soldiers during and after wars, and has previously been called battle fatigue. |
|
See how 2 Wikipedia editors have cleared the way for Simon Wessely to get the credit for my ideas and research here. |
| The real man | The straw man | The counterfeit man |
| I proved that CFS was a real physical condition and developed exercise and other methods of treatment etc. | Two Wikipedia editors described me as a worthless, non-notable fringy kook whose ideas were nonsense and rubbish | Simon Wessely copied my ideas and methods and has been given a prize and knighthood for his contributions to medicine. |
Creativity and innovation are supposed to be rewarded
In modern civilised society creativity and innovation is encouraged and rewarded because it is recognised that without it a log would still be a log, without being progressively changed into a wheel, and then a wheel into a cart, and a cart into a car.
Without innovation we wouldn’t have had the products of the industrial revolution or the computers of today.
The people who develop new ideas get the credit, and inventors get patents, and authors get copyright which gives them a monopoly to make money from their product or from the licences which they grant to others to manufacture and profit on their behalf in exchange for a percentage.
For that reason drug companies pay millions of dollars to scientists to invent medications that relieve or cure disease, and they get patents and have the drugs carry the name of their company, and they charge a fee for every packet of pills that is sold, and the owners or shareholders in the company make billions of dollars in profit every year, and every doctor who prescribes those pills gets a consultation fee for recommending it. Furthermore, that company has the protection of the law, and anyone who copies the formula can be banned from making those drugs in the future, and fined or jailed etc.
Furthermore, anyone who makes slight alterations to the original successful method has to acknowledge the source and pay a fee as well.
I can prove that I was involved in exercise research for chronic fatigue in 1982, and that it was successful, and that the success is recorded in newspaper reports, and, of course, if the formula or design was wrong it would not have succeeded. Also, I still have a copy of the original research paper in which I recorded the results
I knew that some people would try to copy it, and take the credit for developing the method, and profit financially from it, because any method which did not use my principles was guaranteed to fail, but I didn’t know exactly who, or how it would be copied.
Somebody has copied it, and others have copied the copy, perhaps without knowing that I was the originator of the method, so that it is now used all around the world under the names of PACING, and Graded Exercise Therapy.
I haven’t made any money out of that research, but many other people have, by repeating or confirming that research, and by charging a fee for running such exercise programs, and by charging a fee for giving the advice to patients, and millions of patients would have benefited from it by acquiring a better ability to manage their symptoms.
The denial of my rights, and the use of my methods without paying me a fee is a crime.
However, two anonymous Wikipedia editors have described me as a non-notable fringy kook whose ideas are nonsense, and yet Simon Wessely, who has copied my ideas deliberately, or inadvertently without knowing the source, has been given the John Maddox Prize for courage in science?, and a Knighthood for his contributions to medicine.
I have had a comment directed to me which is essentially this . . . “Too bad sucker, that’s life, get used to it“.
Civilised society is supposed to encourage innovation????
Why my research paper was not published
When I designed the exercise program for chronic fatigue patients in 1982, I knew that it would be successful before it even started, and when I was asked to repeat it for another 12 weeks, and again for a third time, I knew that I would be confirming the same results.
I also knew that it would be very easy for anyone else to copy the method and claim the credit for it, so I needed to get it published to prove that I had done it.
However, I was not a doctor and had not been taught how to prepare articles for journals, so I just presented it in the general style that i saw in the research literature. I then discussed the matter with the head of the institute and asked him if one of the research cardiologists would edit it for me to make it fit with medical publication format. He later advised me that they were too busy on other projects, so I posted it to two journals. One sent a standard reply that they receive many manuscripts and that mine wasn’t included in their small accepted list, and the other one sent me a polite reply about the merits of the study, but added that he couldn’t publish it because it didn’t meet their format.
I was then fully aware that anyone who was familiar with what I had done would be discussing the success of the project at local and interstate medical conferences, and talking about how I achieved success, and that anyone who wanted to copy the idea could easily do so and claim it as their own, unless I had something published to prove it was mine.
I did the research for free, so I didn’t have much money, and couldn’t afford to pay a professional academic writer to prepare the article in the formal style. I then managed to find out about an interstate freelance journalist, and phoned him to discuss the project. He asked me to provide the name and phone number of the head of the research institute to confirm that what I said was true, and then wrote an article.
I assume that he sent it to all major interstate and international newspapers, but the only ones I could find were those which were available at local newsagents and included the West Australian. the Sydney Morning Herald, and the Courier Mail in Queensland.
I then put the research paper into my filing cabinet where it stayed for about 25 years until I joined Wikipedia and two of the anonymous editors described me as a non-notable fringy kook, and my ideas as stupid nonsense.
I therefore scanned copies of my original research paper and put it on my website as evidence and proof that my research process was conducted in the proper scientific manner.
I also found that while the two editors were criticising me, they or their anonymous friends were also rewording my ideas and putting them into other topic pages, and then noticed that other people in the research world have been doing the same.
They will also be exploiting the fact that my actual research paper was not published, and be making all sorts of other excuses to justify their actions.
It is possible that many of the people who are using those methods nowadays don’t know where they actually came from, but nevertheless, they are my methods.
I proved the concept.
There is more than one way to prove that my methods have been copied
The proof of plagiarism would usually be me providing a publication of my research in a medical journal, and showing that Simon Wessely did the same.
However, my paper was not published, so the proof is as follows
1. If it was just an ordinary idea the head of the IFRT would not have accepted it as a project
2. If I didn’t know what I was doing I would not have been invited to design the type of exercises, and to co-ordinate the project
3. A newspaper article was published which shows the type of fatigue patient who was invited to attend
3. If the exercises were not designed properly the patients would not have started or continued.
4. If some of those patients completed the 12 week course it was proof of success.
5. The follow up newspaper article is proof of success
6. Follow up news articles were published as recruitment articles for the second trial, which is further proof that the first was successful, otherwise, if it failed why would the institute do it again.
7. Further follow up reports were published in newspapers etc which further proves success.
The exercise principles which I developed were successful, and any other type would fail, so mine had to be copied.
For example, Simon Wessely’s program had to involve gradual exercise, otherwise too rapid an increase would have resulted in a 100% drop out rate.
Wessely’s program also has to specify that if the person had problems with symptoms they should slow down, stop or rest etc. otherwise there would be a 100% drop out rate.
By contrast, if he copied my principles precisely he would have gaines success from sufficient numbers of patients to make it worthwhile, and he would have gained the same range of success, from those who didn’t start, to those who completed 12 weeks or more and stayed the same, improved or returned close to normal levels.
Simon Wessely could have deliberately stolen my ideas and play dumb, and not respond at all, in order to create the impression that it is not important enough for him to bother with.
He could ignore my suggestions that he copied my idea and hope that the issue of copyright theft goes away
He could claim that he invented the ideas himself, or that he developed them from other sources etc.
He could say that he had never heard or read anything about my ideas, or my essays or books, or my website.
He could even acknowledge that he has recently became aware of my comments and happily link to my ideas, accredit me as the developer of the first reliable method of understanding and using the exercise method.
However, what he can’t do is change the fact that I actually did do the research project in 1982, and it has been published in a sufficient manner and frequency as to prove that I actually did get it right.
Other people could argue that my ideas are simple, but they would not be aware of the previous misunderstanding of the aiment where the fatigue was regarded as “just normal” or due to laziness, the lack of exercise, or the fear of exercise etc. or the previous advice that all the person had to do was to join an exercise class and keep going until they got well etc. They also would not be aware of the time and detail in my descriptions of the fatigue in relation to exercise and other aspects of general living which no-one has previously noticed or understood.
Read how Semmelweis was ridiculed and driven mad for developing the antiseptic method for preventing disease here.
emb
|
A quick and precise summary of my method and how it has been copied If you want to know how Simon Wessely has copied my method then you can check the various types of wording of his reports yourself, but first you will need to read what I have to say below, so that you know what the procedure was before I started, and why it failed, and why I succeeded, and why other people have been copying it since. 1.The method of treating chronic fatigue with exercise was to gradually improve the level of exercise from week to week until the person returned to the normal fitness levels of good health, but the patients would drop out of the courses and nobody would be left to assess the results. That method made it possible for the patients to continue training for 12 weeks, and hence it was possible to scientifically measure their fitness levels again and learn the affects and benefits of exercise.
As you can see, they have used different words to describe that method of training, but it is an exact copy of the method which I developed.
“(a) no sprinting or accelerating I knew that all sorts of people would copy the idea and try to take the credit for it as soon as I put it in writing and proved it. The standard method of testing the effects of exercise Up until 1975 there was a standard method of testing the effects of regular exercise on patients who had a wide variety of health problems, such as ashtma, arthritis, and obesity etc. It involved scientically testing the aerobic, or fitness capacity of each person before they started training, and was followed by fitness training for one hour twice per week for 12 weeks. Each session included 20 minutes of light exercises such as arm movements and bending to touch the toes, and 20 minutes of walking or jogging, and 20 minutes of rest or other activity. They were also encouraged to gradually increase the level of exercise each week which meant heavier exercise, more often, and faster walking or running, for longer distances. At the end of 12 weeks their fitness levels were scientifically measured again to assess the effects of the regular exercise Many people who had asthma or arthritis etc would complete the course, and it was found that the exercise improved their health, but, at some stage or other, all of the people with chronic fatigue were dropping out of the training before completion, so it was not possible to determine the effects. My method In 1975 when I actually had chronic fatigue, my doctor couldn’t explain it, or treat it, and I had absolutely no knowledge of medicine, so I decided, on the basis of common sense, that I might be able to cure the problem by exercising at low levels first, and gradually increasing the levels of exercise each week until I returned to normal health. However, I found that when I tried to keep up with other people I would get difficulty with various symptoms inclucding breathlessness, so I slowed down to levels which made it possible to continue, and kept training for almost a year. A few years later, I was reading the medical literature and found out that researchers were having difficulty getting other fatigue patients to train. More years went by when I was introduced to the head of the research institute in Adelaide and explained what had happened. He then asked me to design a method of exercising specificlally for chronic fatigue patients and co-ordinate a research study. 25 people were tested, and 6 people trained for 12 weeks, and continued for another 12 weeks, which proved the concept. That concept became the standard method which is now used all around the world. Since then I have become interested in the history of medicine, and there have been other people who have used all sorts of exercise methods as a treatment with varying degrees of success. I defined that method clearly, and it has since been standard practice. See also here Another set of time frames on the copying of my research methods 1976: I invented the method of exercising to treat my own chronic fatigue, by starting at a low level, and gradually increasing at my own rate and within my own limits. 1982-1984: I scientifically proved that it was possible to have other chronic fatigue patients train for 12 weeks, and then 24 weeks or more, at the South Australian Institute for Fitness Research and Training. The success of the program would have become widely known in the research community, and was widely reported in South Australian and interstate newspapers. 1987. Simon Wessely. of London, England, began his interest in undetectable illnesses such as chronic fatigue syndrome, and it’s definition, and treating it with a method which he called “Graded Exercise Therapy” where the patients were required to remain at levels where they did not become fatigued. 1993-2000: I wrote a book about health in 11 editions at the rate of 150 pages per year until it became a thousand pages of detailed information about my ideas, including more than 50 pages related to chronic fatigue, and more on battle fatigue, & more on the related symptoms, and how it is completely different to normal fatigue etc. I also set up a website for similar purposes. 2001: I sold the final 1005 page printed edition of my book, the 11th edition, to libraries in Australia and New Zealand. From that year Simon Wessely would have nothing more that he could copy. The following words are a quote from a report in The Times on 6th August 2011, by Stefanie Marsh, after her interview with him . . . “ten years ago, Professor Wessely chose to give up his research” (end of quote). His excuse was that patients were harassing him because he is a psychiatrist, but the real reason would be that without my detailed descriptions and analogies he would have nothing more to copy. I note that he is still using double talk and telling a lot of lies about the nature of the problem, for example, by arguing that it’s chronic nature relates to the patients perception of the condition, when in fact, he knows that it had been recognised as a chronic condition long before the modern media started writing about it, and long before patients knew anything at all about it. See here. 2007-2009: Two Wikipedia editors argued that my research and methods were non-notable, because it was not published in medical journals, and that I was not an academically qualified person, but was just an exercise “technician” in one, minor, research study which did not warrant any mention at all in Wikipedia, and deleted it, and all links to my website, and arranged for me to be banned, but some of the bests of my ideas remained on the page, or was transferred anonymously to other related topic pages, without any mention of my name, books, or website. In the meantime various editors had asked me to provide proof that I actually did the research. I then searched through my 30 year old files and found the actual research paper, and scanned it’s pages which contained the actual details of the method and placed it on my website on 17-1-2008. I later scanned a copy of a newspaper article onto my website, and they argued that it was proof that I had a conflict of interest , and deleted it for that reason. 2009-2011: I began criticising the two editors who were nitpicking my contributions, and provided proof that they were both telling lies about me, the rules, the topic, and the reliability of my references. I also added scanned copies of other newspaper articles as proof that I had designed the 1982 research method. November 2008. A colleague of Wessely’s named Peter White had internet access to all of the details of success, and completed recruitment for a research project called the PACE trials, in which he studied the relationship between the chronic fatigue syndrome and exercise on a larger scale of 640 people. 2012: Simon Wessely was awarded the John Maddox Prize by “Nature” magazine, and the “Lancet” medical journal for his courage in science relating to his research about the chronic fatigue syndrome and “graded exercise therapy”. 2013: Simon Wessely was knighted for his contributions to medicine for closely related reasons. 2013. Peter White announced the publications of his Pacing trials with conclusions that were similar to mine from 1982-4. Summary 1982-1984: I scientifically proved my exercise methods for chronic fatigue at the South Australian Institute for Research and Training, but was unable to get my research paper published. 1987: Simon Wessely had the opportunity to learn the general principles which I developed, and began his research into chronic fatigue syndrome and exercise. 17-1-2008: I added scanned copies of newspaper articles about the 1982 research project, and the scanned copied of my unpublished research paper, which contained all the details on how to run the program efficiently. November 2008: Peter White had instant internet access to all of the details on my methods of success from 1982, and began a larger scale study of 640 chronic fatigue patients called the PACE trials and their response to exercise, and completed his report which was essentially a repeat of my methods, results, and conclusions, but on a larger scale. 2012: Simon Wessely was given the Simon Maddox Prize for his study of chronic fatigue syndrome and “graded exercise therapy”. 2013: Simon Wessely was knighted for his contributions to medicine, and Peter Whites paper on Pacing trials was completed and published. Verifying information about Simon Wessely’s biography Verifying information on the biography of Simon Wessely and when he started etc, can be seen here. These are a few quotes . . . “I am currently the Chair and Head of the Department of Psychological Medicine at the Institute of Psychiatry, King’s College London. I am also a Consultant Liaison Psychiatrist at King’s and Maudsley Hospitals, which means that my main clinical work is in the general hospital or seeing patients with chronic fatigue syndrome” . . . and . . . “I became very interested in the general area of medically unexplained symptoms and syndromes, and chronic fatigue syndrome in particular” . . . and . . . “he always intended to study psychiatry, and started training at the Maudsley in 1984” . . . and . . . “His research has covered epidemiology, post traumatic stress, psychological debriefing, chronic fatigue syndrome, history, chronic pain, somatisation, Gulf War illness, military health and terrorism. In the first part of his career his main areas of research focused around clinical epidemiology, and with special emphasis on unexplained symptoms and syndromes, most particularly the chronic fatigue syndrome. He established the first NHS only service for sufferers, and the first academic unit in this country dedicated to researching the illness. Over the years the unit has produced research looking at many aspects of the illness, including biochemistry, epidemiology, history, immunology, neuroimaging, neurology, psychology, psychiatry, sociology, virology and other areas” . . . and. . . “Finally, he has recently co authored books on chronic fatigue syndrome, the randomised controlled trial in psychiatry, and a new history of shell shock– but none has yet reached the best seller lists” (end of quotes) See here. Two Wikipedia editors cleared the way for Wessely to take the credit for my 38 years of research I would suggest that his book will contain a neat summary of all of my detailed observations, descriptions, ideas, methods, research, and theories, but he will give the impression that he or his local and international colleagues thought of it all. Between 2007 and 2009 two anonymous Wikipedia editors defamed, discredited and deleted all information about me, and my research, and made it clear that no link to me would remain. That process has made it a clearway for Simon Wessely to write his book, and the history of research as if I never existed, and as if he and he thought of it all. I have recently discovered, that while the 2 editors were criticing me, they knew exactly how valuable my ideas were, because, apart from other considerations, there is a Wikipedia page on the biography of Simon Wessely, and while I am not mentioned anywhere, he is free to get all of the credit for every method which I developed.. What two Wikipedia editors did to hide my research ideas and methods While I was contributing information to Wikipedia I was confronted by two anonymous editors who described me as a non-notable fringy kook who was writing rubbish and nonsense. They argued that there was nothing in the “real” medical literature about my ideas, and that I was just a sports technician who was involved in one minor short term insignificant study which did not deserve even one sentence in Wikipedia. They accused me of breaking almost every rule in Wikipedia, told massive numbers of lies about me, my ideas, and my references, and arranged for me to be blocked from adding any information from any source, and they eventually had an admin use Wikipedia’s “ignore all rules” policy to ban me. In the meantime they deleted most of the top quality information on a page about Da Costa’s syndrome, but kept my description of how to treat it, which was based on my own experience and theories. Also, at the same time, and later, after they deleted the information to the pages where I added it, they transferred it to other pages about “postural orthostatic tachycardia syndrome”, “orthostatic intolerance”, and “costochondritis” etc. In other words they have kept virtually all of my ideas because they know that they are the best which have ever been written on the topic, but they don’t want anyone to know where they came from. They were deliberately insulting and offensive to defame my character, and discredit me personally, which brings up the question of why. While I was writing my descriptions and methods I knew that other people would be tempted to steal them, and from time to time I had indirect evidence of it. However, recently I have found out about Simon Wessely, and his prizes and knighthood for his contributions to medicine. I began my research between 1975 and 1982, and continued it with my book between 1994 and 2000 and my website, and Simon Wessely started in 1987. He and his colleagues have been copying me ever since, with him as the ring leader. My two critics who were continually pestering me in Wikipedia obviously knew that, and they did everything they could to remove my name from Wikipedia, so that Simon Wessely could get the credit for all of my ideas. Wikipedia has a biography page about him, and it refers to him starting his interest in medically unexplainable symptoms and chronic fatigue in 1987, and helping to improve the definition, and they refer to his research papers and books on chronic fatigue, and his interest in the problem amongst soldiers, and in medical history. He is also referred to as the person who developed and studied the concepts of graded exercise therapy, pacing, and cognitive behavioural therapy. He started by arguing that the symptoms were mainly somatisation (imaginary or caused by the mind), and is now portrayed as a man who is trying to help patients deal with the stigma by arguing that it is a physical illness. This is what Wikipedia said about him from 26th August 2005 “Simon Wessely is Professor of Epidemiological and Liaison Psychiatry at King’s College School of Medicine, London, UK. This is what they said on 14th November 2005. “Wessely has established an unrivalled position as a well placed government adviser and peer reviewer in almost all the seminal journals. He has been involved with every serious inquiry into ME and CFS over the past decades, and his papers and those of his colleagues, produced in considerable number, dominate the field in any literature review.” See here. This is what they said on 29-1-2013 “Wessely and his colleagues, using randomised controlled trials and follow-up studies,[13] developed a rehabilitation strategy for patients that involved cognitive behavioral and graded exercise therapy, that is effective in reducing symptoms of CFS (a condition that otherwise lacks a cure or unequivocally successful treatment) in ambulant (non-severely affected) patients.” here. I am the person who developed those ideas in great detail, and Simon Wessely is just a copycat. He has made his research career out of my ideas. However, Wikipedia portrayed me as a fool, and Simon Wessely as the hero of modern medicine. See my research paper here . . . and my chronic fatigue/exercise research summary added to Wikipedia at 5:58 on 18th December here. It was deleted at 1:34 on 14th January here.
|
From The Cambridge History of Medicine
The attitudes toward chronic fatigue before I wrote my theories
In the 19th and early 20th centuries people who suffered from pain and fatigue or paralysis were diagnosed as having ‘nervous spine’, ‘neurasthenia’ or ‘fits’. Edward Shorter called such people “somatizers” and described them as suffering from “pain and fatigue that have no physical cause“, and suggested that they were playing sick as a means of consciously or sub-consciously seeking solace, attention, or social excuses. “Such somatizers have produced a fascinating succession of phantom diseases” and the “Archetypal Victorian ladies” collapsed on their beds, or had fits, convulsions, or paralysis, but, “By 1900 such operatic displays softened into a symptomatological chamber music”, of less dramatic symptoms of neuralgia, headache, and fatigue. Such patients were “frustrating to no-nonsense physicians such as the early twentieth Kentucky doctor who believed that “a good spanking”, or sometimes even a “good cussing” was the best treatment for such “evident hypochondriacs”. Nowadays the condition is called “myalgic encephalomyelitis or ME (also called ‘yuppie flu’ or Chronic fatigue syndrome)”. Reference: The Cambridge Illustrated History of Medicine (1996) p.111-112 See my full report on the history of treatment here.
Simon Wessely is a research Identity theft
Who is the hero, and who is the villain
Anyone who agrees that a former gymnast who developed CFS would invent an excise method for regaining fintess is being sensible.
Anyone who believes that a psychiatrist would develop a physical exercise method for treating CFS is being utterly thoughtless, dumb, and gullible.
Since 1975 I have been researching and describing, in detail, the physical basis for many undetectable illnesses which were previously regarded as imaginary or mental disorders, in particular chronic fatigue. I have also developed and defined methods of treating the problem which includes modified exercise programs and other ways of managing the symptoms. Nevertheless, I have, at times, been ignored or criticised in quite a hostile manner. During that time another person named Simon Wessely has been copying, or stealing my ideas, and claiming them to be his own.
However, a small group of Wikipedia editors, and others, including some of Simon Wessely’s colleagues, have been conjuring up some carefully crafted spin to portray him as the hero of modern medicine, and me as the villain. He has been awarded several prizes, and been knighted for his contributions to medicine, whereas I have been portrayed as a non-notable fringy kook, and a disruptive troll whose ideas are worthless rubbish and nonsense.
In fact, if anyone is the hero it is me, and Simon Wessely is the villain.
The history since my research of 1982-3
See my research paper, followed by my subsequent comments here.
When I designed a reliable exercise method for chronic fatigue, and scientifically proved that it as a physical condition in 1982-3, there have been major changes. The CDC of the United States officially listed the “chronic fatigue syndrome” as an illness in 1987, the U.K. government started providing funds to research the effects of exercise in chronic fatigue syndrome patients to the amount of more than eleven million dollars, and there have been many thousands of research papers published on the subject of CFS and exercise.
Here are a few examples . . .
“In 2000, a Belgian/Australian collaborative study entitled “Exercise Capacity in Chronic Fatigue Syndrome” was unequivocal: “Comparing the exercise capacity in our patients with data from other studies shows a functionality similar to that of individuals with chronic heart failure, patients with chronic obstructive pulmonary disease, and those with skeletal muscle disorder”. Specific findings included (i) the resting heart rate of patients was higher than controls but patients’ maximal heart rate at exhaustion was lower than controls (ii) the maximal workload achieved by patients was almost half that achieved by controls (iii) the maximal oxygen uptake was almost half that achieved by controls. This would affect patients’ physical abilities, leading the authors to comment: “This study clearly shows that patients with ME/CFS are limited in their capabilities”. Taken together, these findings “suggest that alteration in cardiac function is a primary factor associated with the reduction in exercise capacity in ME/CFS” (P De Becker et al. Arch Intern Med 2000:160:3270-3277).” and . . .
“In October 2004, at the 7th AACFS International Conference held in Madison, Wisconsin . . . Spanish researchers (Garcia-Quintana) presented their work on aerobic exercise, providing evidence of low maximal oxygen uptake in ME/CFS patients. This confirmed previous studies showing that patients with ME/CFS have a markedly reduced aerobic work capacity on bicycle ergometry.” and . . .
“In 2005, Black and McCully published their results of an exercise study in patients with ME/CFS: “This analysis suggests that ME/CFS patients may develop exercise intolerance as demonstrated by reduced total activity after 4 – 10 days. The inability to sustain target levels, associated with pronounced worsening of symptomatology, suggests the subjects with ME/CFS had reached their activity limit” (Dyn Med 2005: Oct 24: 4 (1): 10).” and . . .
“Black and McCully’s results concur with those of Bazelmans et al that were published in the same year. That study examined the effects of exercise on symptoms and activity in ME/CFS: “For ME/CFS patients, daily observed fatigue was increased up to two days after the exercise test. For controls, fatigue returned to baseline after two hours. Fatigue in ME/CFS patients increased after exercise” (J Psychosom Res 2005:59:4:201-208).” and . . .
“For all three PACE Trial PIs to have known conflicts of interesa about one of the interventions supposedly being tested in the PACE Trial and to be publicly known to be strongly opposed to that intervention casts serious doubt on the validity of their finding that pacing does not work.
It is therefore necessary to be aware that Adaptive Pacing Therapy (APT) used in the PACE Trial is very different from pacing as practiced by patients with CFS/ME. APT as used in the PACE Trial is a vehicle for incremental aerobic exercise and involves planning, achieving and sustaining targets. The CBT Therapists’ Manual states about APT: “Activity is therefore planned”, which indicates a structured activity regime, and the APT Therapists’ Manual lists other requirements for APT including “plan set activity in advance” (so activity must be “set activity”, not simply what the patient may be capable of doing at the time); there must be “activity analysis”; APT participants must “constantly review model, diaries and activity” and there is the requirement to “involve relatives”, which is nothing like pacing, ie. “doing what you can when you can”.
The Lancet article seriously misleads readers because the authors state: “Our results do not support pacing, in the form of APT, as a first-line therapy for chronic fatigue syndrome”. From his published record, Professor White was never going to support pacing, but it is improper to refer to APT used in the PACE Trial as “pacing”; the two are not the same, and other impeccable research (for example, Professor Leonard Jason et al; AAOHN May 2008:56:5) has found pacing to be beneficial for people with CFS/ME. This is yet another example of how duplicitous the PACE PIs have been.
The Minister went on to say: “Various noble Lords have paid tribute to the quality of the research”; they did, but their comments are without foundation, as the Countess of Mar and the international CFS/ME community are keenly aware.” (end of quotes) here.
The correct method of Pacing
The correct method of exercise training for chronic fatigue was invented by me in 1975, and has replaced all others because it is the only one which is effective and is . . . train within your own limits, not other peoples limits, and not prescribed limits. i.e. “doing what you can when you can“. re: the WM
The biased or falsified histories which avoid mention of my research and the change in direction in 1975, and after 1983
There have also been various histories written about the topic. Some of them trace it from 2012 back to 1987, and then stop. Others trace it back from the virus theories of cause in 2012 to the virus theories of the early 20th century and beyond, and miss the 1982-3 period, and some of them start in the 19th century, and miss the 20th century entirely, except for comments that it was classified as a neurosis in the mid 20th century, with the comment that now there is a more accurate and precise understanding of various aspects of the disorder.
Dr. Oz announces a revolution in medical culture on 20-3-13
In 1975 I had been told that none of my health problems were evident on medical diagnostic tests, and it had been implied, and in some cases stated that the symptoms were “all in my mind”. The widespread implication of that time was that such patients were “hypochondriacs” who complained about nothing.
I began looking for a more realistic cause and within five years was able to write an essay on the physical basis for those symptoms which I have since called The Posture Theory, and in due course spent another six years writing a thousand page book by that title. One of my objectives was to provide so much evidence of a physical cause that it would be impossible for any doctor, or any psychiatrist to argue that any patients with undetectable pain were hypochondriacs in the future.
On 20-3-13, on Channel 7 Television, Adelaide, Dr. Oz, on his show, introduced many of the audience members who had described how they had been to their doctors and been told that their pain was “all in the mind”, or that they were just depressed, or after drugs, and that they were the victims of prejudice etc. However he didn’t mention the label of hypochondria.
He then announced a new cultural revolution which was happening in medical practice based on a ground breaking discovery that pain was a disease in it’s own right which could occur because of memories in the brain which persisted after wounds in the body had healed. (I don’t wish to comment on that idea).
However he said that the main problem was that doctors couldn’t “see” the pain, and that many of them still believed that their patients were crazy, but that they were wrong, and needed to be educated to recognise that the pain was “not” all in the mind, but was real, and physical. He added that there was no such thing as a “pain-o-meter” which could accurately measure the severity of pain, and that it was whatever the patient said it was.
He also said that the pain came first, that naturally, depression was a common result, not vice versa.
He then says that he is calling on patients to help doctors in understanding their diseases.
I have already been describing such ailments in detail for 37 years, to help doctors and patients understand those ailments more realistically, and treat them more effectively, and remove the prejudice and stigma.
However, I have mostly been ignored, and two editors have described my research and books as non-notable nonsense and rubbish which does not deserve even one sentence in Wikipedia.
Now, Simon Wessely, and Dr. Oz are doing what I started and made inevitable, and they are famous, but most patients have never heard my name, and many people obviously don’t want them to know that I ever existed.
It was doctors and psychiatrists who created the “all in the mind” ideas, and the problems and prejudices, and they don’t want the public to know that a patient proved them wrong.
They want the public to believe that they, the new doctors, have removed an old problem themselves.
See the webpage about my theory here, and about the physical basis for hypochondria here, and the cause of undetectable abdominal pain here, and my eBook on the cause of undetectable physical illnesses here.
A Summary of the Changes in opinions about chronic fatigue 1975-2013
People who copy my methods, or steal the ideas by claiming them to be their own do not deserve respect, and those who find out about it, and allow other people to get the credit, don’t deserve my help.
All I can say is that the copies are not as good as the original, and copyright thieves are like photocopy machines. Without the original, all you have got is a blank piece of paper, and that is all you get out. See my report on copyright thieves above and here.
In 1975 I had many problems with my health, and my doctor said that he didn’t understand them, and that left me in a position where I decided, at the age of 25, that I didn’t want to spend the remainder of my life like that.
I soon found that the symptoms were generally regarded as no different to those experienced in healthy people, but that the patients were supposedly concerned excessively about the sort of problems that normal people wouldn’t complain about, so I decided to write about them in detail, to make the differences clear. See a list of my publications here.
Seven years later I was invited to design a research project to scientifically prove those differences at the South Australian Institute for Fitness Research and Training, which I did.
The following chart shows the ideas which dominated world opinion before I did my research in the left column. The centre column shows one of many newspaper articles which reports the success of my research project, and the right column shows all of the details which I wrote, and all of the methods which I used in that project, but they have since been copied by other people, who have not acknowledged me as the person who developed them, but they can be seen in all modern reports thirty years later, in 2013, in research papers, books, encyclopedia’s and official definitions and guidelines about the chronic fatigue syndrome, and surveys of patients has shown that they are regarded as the most effective form of treatment available today.
|
Before my research started in 1975 |
News of my research success 1982 |
Modern methods 2013 |
|
1939 . . . “The typical patient with the ‘effort syndrome‘ was “”never allowed’ to take part in competitive sports” and has felt inferior physically to others of his own age”. . . “They never learned to keep on when the going was hard” . . . during the exercise test . . . “the response is no more dependent on the amount of exertion as it is than on the emotional reaction he has, the fear that he has that the test will injure seriously his already weakened heart” Reference: Caughey J.L. Jr. M.D.(April 1939) Cardiovascular Neuroses: A Review. Psychosomatic MedicineVol.1, No.2, p.311-324. see my full report here 1974 . . . “attempts by Cohen and his associates to alter these abnormalities by physical training were unsuccessful since the patients could not or would not follow the prescribed training programme.” Hurst J.W.: R.B.Logue, R.C. Schlant, N.K.Wenber (1974), The Heart 3rd. edition. New York: McGraw Hill Book Co.,, 1552-1555. |
 |
The recommendations which I made, and which are now the most effective form of treatment were. 1. Chronic fatigue is a real physical condition. 2. Some people benefit from an improvement in their fitness and health if they follow these instructions 3. Begin at a low level, 4. Exercise at your own rate (or pace). 5. increase the levels of exercise very gradually over a period of weeks or months. 6. If you experience any symptoms at the higher levels of exercise, determine what that level is, and try to stay below it. 7. If you have problems, drop back to the level which is not causing problems and rest for awhile if necessary, or take a couple of days off and resume again later. |
Needless to say, that my methods of exercising have improved a lot in the past 38 years, and I don’t have any problems in determining what to do. However, modern research programs are reporting that 51% of patients are worse off after the training that they were before, and some have become permanently incapacitated.
While copyright thieves are stealing my ideas and methods, and being given the credit, and the funding, and all the other related benefits, and while other people are not acknowledging that it is my methods, it is simply not worth my while to tell them what they are doing wrong, or how to correct all of their mistakes.
I could do that, but there is no guarantee that those ideas wouldn’t be stolen as well, so the only practical thing to do is to keep the methods to myself until I am given the credit for what I have already done.
I now write all my ideas and methods in code. See here.
How to solve the problem
If my research paper from 1982 was published in a top quality modern research journal, then I would be able to make it clear that I developed those methods, and then I could consider providing improvements to the methods as long as they were also publshed in research journals soon after, not 30 years later. See here.
What modern CFS patients need to know
When I asked my doctor what to do in 1975 he would shrug his shoulders in confusion and say he didn’t know. One of the suggestions that I was given later was to go to a small house in the suburbs where several older, middle aged men were sitting around a table and sticking icecream sticks together with glue to make small model cars and houses. It was called occupational therapy. They all looked miserable and bored so i never went back.
I kept on doing my own research and developing my own methods of treatment which almost everyone now copies.
When you watch the discussions amongst CFS patients today, they are discussing whether to do exercise or not, what to do, when to do it, and how to do it, and what to do if they have problems, and they do the same things about their problems in life in general.
The main change I have noticed is that they are not asking each other to pass the glue.
The label discussions about “chronic fatigue syndrome”
When I started studying my own symptoms I soon found that I had “Da Costa’s syndrome”, and a few years later when I asked a research cardiologist what the formal medical term was he said “neurocirculatory asthenia”, and when I started reading the research journals I found that it had at least six common names, and more than 100 in the past century of research where countless people have attributed it to almost every cause.
In 1982, Tony Sedgewick asked me to design and organise a research project to study the effect of exercise on patients with that ailment, where fatigue, and problems with exercise were the main identifying symptoms.
One of the first tasks was to make patients aware of the project and invite them to participate. I therefore contacted a newspaper journalist named Diane Beer. She asked me the name of the ailment, and I had to consider that most people with the problem didn’t known that it was called Da Costa’s syndrome or neurocirculatory asthenia etc, so I chose the word “neurasthenia” as the least jargonistic, and then told her that we needed people who had long term problems with persistent or recurring abnormal fatigue.
By 1983 I was able to scientifically prove that it had a physical cause, which replaced the old ideas that it was imaginary or psychological. and that a properly designed exercise program could help some of the patients, and the success of the project was widely reported in major interstate newspapers throughout Australia and probably internationally.
A few years later I heard people on the radio talking about a supposedly “new” illness called “the chronic fatigue syndrome“.
By that stage I knew a lot about medicine, and that diseases don’t just come from nowhere, but are often just new labels for old ones, and the discussions made it reasonably clear to me that they were referring to Da Costa’s syndrome.
I also knew that after I had proven it was a physical ailment, and not a mental problem, that someone would probably change the label to indicate a clear physical, rather than mental cause, and from what I have learned since that is why the change occurred.
I also eventually discovered that only four years after I had scientifically proven that Da Costa’s syndrome was a physical condition, the U.S. Center for Disease Control and Prevention recognised the label of CFS as a new item.
I had also been curious about who, and why the label was first invented, and at one stage I read that it was coined by a U.S. naturopath in the 1950’s and he attributed it to overwork.
As I said there has been more than 100 labels used for the same illness in the past 100 years, and their have been many heated arguments between those who believe one cause or another, with the most hostile insults being freely tossed about, and some even reporting death threats,
I actually thought that the label of Da Costa’s syndrome was the best at the time because it was named after the man who first identified it clearly, and because it didn’t give bias to any one of the unproven causes.
I also thought that the chronic fatigue syndrome was one of the best because it identified that there was s physical and not a mental condition, and involved an abnormal response to exertion as it’s main feature.
However, some people have been criticising that label because, in their opinion it confuses “normal” “tiredness” with the more disabling medical ailment.
However, when I started studying this problem in 1975 nobody I knew had ever heard of Da Costa’s syndrome, and yet it was a common ailment which affected 2-4% of the population.
The chronic fatigue syndrome is the same ailment, and affects the same number of people, but nowadays everybody has heard of it, and knows that it is a lot different than normal tiredness.
There were many reasons why patients or the public didn’t know anything about it in 1975, including that fact that Da Costa’s syndrome was an obscure label, and, for example, “neurocirculatory asthenia” was too difficult for most people to understand, remember, or pronounce.
By contrast everyone can understand, and pronounce, and discuss the label of Chronic Fatigue Syndrome, in self help groups, and at conferences, and on the radio, and they can confidently expect to be understood.
However, many people want the label changed, and most of those prefer “myalgic encephalomyelitis”, because they favor the virus, or the effect on the immune system as the cause, and are researching that aspect in the hope of finding a cure.
I have been a aware of that possibility, and at one stage in the mid to late 1980’s I attended a self help group called the chronic fatigue society where a woman was discussing the possible viral cause. I had my own ideas at that time, so I didn’t want to argue, or even join their group, but on the basis that two heads are better than one, I thought to myself that it was a good thing that I was not the only patient trying to solve the problem.
However, the current people who are favoring that idea prefer the label of Myalgic encephalomyelitis, so I will make some comment which are meant to be useful and constructive.
When I added information to the page about Da Cotta’s syndrome to Wikipedia two of their anonymous editors obviously didn’t want the readers to know the facts, so one of their ‘tricks’ to get the idea lost, was to delete it, but another was to invent a new page called “Somatoform autonomic dysfunction“. That label means “imaginary illness” or “hypochondria”, but it is also the type of complex jargonistic name that no ordinary patient is going to find or criticise, which is why those two editors wanted to use it
The process of looking for causes and cures is good, but I think that changing the label of myalgic encephalomyelitis could cause a similar problem of driving a now well known and studied ailment back into scientific and public obscurity.
To illustrate what I mean, I can give the example of asking an ordinary person what the word chronic fatigue syndrome and they will be able to tell you something about it, and that it is different to normal fatigue, and that some of their friends, or people they have met suffer from it.
By contrast, if you ask them what the know about myalgic encephalomyelitis they will possibly ask you to say the word again, or repeat the question, but are more likely to say “myelo – what” , or “myalgio – who” or “mmmmmm” or myalgio -whosamewhat”.
It is clear that most people are not familiar with medical jargon, so they can’t understand or even say the word the first time.
Using words like that creates the same problem as a Chinese man, speaking Chinese on an Australian TV show and expecting 99% of the population to understand it, when in fact it would probably be closer to one in a million.
I can practically guarantee 200 million patients who have chronic fatigue, that the only reason their condition is so well known today is because I started studying it in 1975, and went through the process of learning the medical language, and then writing about the topic in plain English.
If the two anonymous editors of Wikipedia had their way, the name would be “Somatoform autonomic dysfunction”, and would be classified as a mental illness, and patients wouldn’t know.
I therefore suggest that the name should be kept as the chronic fatigue syndrome, or if it is to be changed, that it be an easily useable term in plain English, so that people understand it.
At the moment one of the most popular names is ME/CFS, which includes the complicated acronym for Myalgic encephalomyelitis, which most people can’t pronounce, let alone understand, and Chronic fatigue syndrome, which lets other patients and most members of the public know what it is – a set of symptoms where an abnormal form of fatigue is the main one.
Horses for courses
Not the only cause, not the only treatment
Additional to the range of causes and treatment options
When I wrote my theory about poor posture being the cause of chronic fatigue I did so on the basis of many years of experience and detailed observations of my own symptoms, combined with a knowledge of anatomy and physiology, and reinforced by independent reports in the research literature. I then wrote about them to help other people understand and treat the ailment more effectively.
However, critics have argued that some patients don’t have that physique therefore the idea is wrong, stupid, or useless and should not be considered.
Similarly, when I developed a method of treating my own symptoms by using mild exercise within limits, critics have argued that some chronic fatigue patients can’t exercise, and some of those who try have adverse effects, therefore the method is wrong, stupid, or useless, and should not be used.
However, the same criticism can be made about every idea for cause, and every method of treatment.
Consequently, my ideas are an additional way of looking at the cause which does actually apply in many cases, and my methods of treatment are additional to the range of other treatments and can be applied where appropriate to improve outcomes where other methods are used, or when other methods are not effective.
A new diagnostic method
In October 2012, I determined an entirely new way of researching and diagnosing the chronic fatigue syndrome, and may report the method later. I call it the Diagnostic Attenuation Study.
For more information about the chronic fatigue syndrome:
The South Australian Chronic Fatigue Society- ME/CFS Australia (SA) Inc.here http://www.sacfs.asn.au
The National Alliance for Myalgic Encephalomyelites here http://www.name-us.org/index.html
An article from the National Alliance for exercise testing here
A website called Doctors CFS page – Chronic fatigue syndrome information for medical doctors here